Download
1 / 37
420 likes | 921 Vues
Assessment of the gastro-intestinal system. Instrumental methods of examination. Introduction. why assess the abdomen in the prehospital setting? abdominal pain accounts for up 10% of emergency visits 15-30% of patients with an acute abdomen will require a surgical procedure. Anatomy.

E N D
Assessment of the gastro-intestinal system. Instrumental methods of examination.
Introduction • why assess the abdomen in the prehospital setting? • abdominal pain accounts for up 10% of emergency visits • 15-30% of patients with an acute abdomen will require a surgical procedure
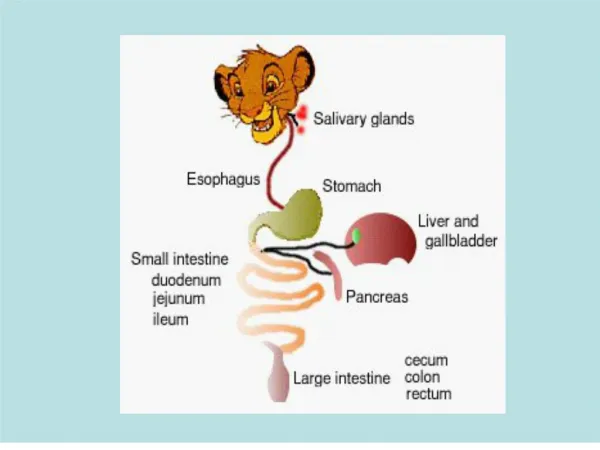
Anatomy • Gastrointestinal system involves the esophagus ,stomach, small and large intestines • They work with the pancreas liver and gallbladder to convert nutrients from food into energy. • Waste is then excreted.
Right Upper Quadrant (RUQ) • diaphragm • liver • gallbladder • kidney • Hepatic flexure -large colon • small intestine Left Upper Quadrant (LUQ) • spleen • kidney • pancreas • stomach • Splenic Flexure –large colon • small intestine Right Lower Quadrant (RLQ) • appendix • large ascending colon • ovary • uterus • bladder • small intestine Left Lower Quadrant (LLQ) • descending colon • ovary • uterus • bladder • small intestine Anatomy - 4 Quadrant System
Right Hypochondriac Epigastric Left Hypochondriac Right Lumbar Umbilical Left Lumbar Right Iliac Hypogastric (suprapubic) Left Iliac Anatomy - 9 Quadrant System See graphic on next slide
Assessment of Abdominal painO-P-Q-R-S-T ONSET • rapid onset of severe pain is more consistent with a vascular catastrophe, passage of a ureteral or gallbladder stone, torsion of the testes or ovaries, rupture of a hollow, viscous, ovarian cyst, or ectopic pregnancy • slower onset is more typical of an inflammatory process such as appendicitis or cholecystitis
Assessment of Abdominal painO-P-Q-R-S-T Provokes / palliates • pain provoked/aggravated by movement, such as hitting bumps on the road or walking is typical of somatic (parietal) peritoneal pain such as that seen in pelvic inflammatory disease or appendicitis • eating often relieves ulcer related pain • eating exacerbates biliary colic – especially fatty foods (usually 1-4 hours following a meal) • Pancreatitis is palliated (relieved) by curling up in a fetal position • frequent movement or writhing in pain is more typical of renal colic
Assessment of Abdominal painO-P-Q-R-S-T Quality • dull, achy or crampy is more likely to be visceral • sharp, stabbing pain is more likely to be somatic or peritoneal • severe tearing pain is classic of dissecting aneurysm
Assessment of Abdominal painO-P-Q-R-S-T Region / radiation • location of pain can vary with time • periumbilical pain that migrates to the right lower quadrant is classic of appendicitis • epigastric pain localizing to the right upper quadrant for several hours is typical of cholecystitis
Assessment of Abdominal painO-P-Q-R-S-T Severity • the patient’s quantification of severity of pain is generally unreliable for distinguishing the benign from the life-threatening • assigning a 1-10 pain scale rating does however allow for a baseline to gauge the patient’s response to treatment • pain that increases in severity over time suggests a surgical condition • Severe epigastric or mid-abdominal pain out of proportion to physical findings is classic for mesenteric ischemia or Pancreatitis
Assessment of Abdominal painO-P-Q-R-S-T Timing • crampy pain that comes in waves is generally associated with obstruction of a viscous • constant pain has a worse diagnostic outcome
Associated signs & symptoms Nausea & vomiting (N/V) • N/V generally associated with visceral disorder • excessive vomiting should raise suspicion of a bowel obstruction or Pancreatitis • lack of vomiting is common in uterine or ovarian disorders • pain present before vomiting is more likely caused by a disorder that will require surgery • vomiting that precedes Abdo pain is more likely a gastroenteritis or other non-surgical condition
Associated signs & symptoms Urgency to defecate may suggest… • intra-abdominal bleeding • inflammation/irritation in the recto sigmoid area • ectopic pregnancy • abdominal aortic aneurysm (AAA) • retro peritoneal hematoma • omental vessel hemorrhage
Associated signs & symptoms Anorexia • intra-abdominal inflammation • common in appendicitis
Associated signs & symptoms Change in bowel habits • diarrhea with vomiting is almost always associated with gastroenteritis • diarrhea may occur with Pancreatitis, Diverticulitis and occasionally Appendicitis • bloody stool indicates GI bleed • constipation or difficulty passing stool or gas may be due to an ileas (impairment in paristalsis) of bowel obstruction
Associated signs & symptoms Genitourinary symptoms • dysurea, urgency and frequency are suggestive of cystitis (inflammation of the bladder), salpingitis, diverticulitis or appendicitis • Hematurea with pain suggests urinary tract infection, but can also indicate renal colic, prostatitis or cystitis
Associated signs & symptoms Extra-abdominal symptoms • myocardial infarction • pneumonia • pulmonary embolus can present with abdominal pain
Assessment techniques • History • Demographic data • Family history and genetic risk • Personal history • Diet history • -anorexia • -dyspepsia
Physical assessment • Mouth and pharynx • Abdomen and extremities • -inspection • -auscultation • -percussion • -palpation
Laboratory tests • Complete blood count • Clotting factors • Electrolytes • Assays of liver enzymes-aspartat and alanin aminotransferase • Serum amylase and lipase • Bilirubin:the primary pigment in bile
Laboratory tests (continued) • Evaluation of oncofetal antigens CA19-9 and CEA • Urine tests-amylase, urine urobilinogen • Stool tests-fecal occult blood test,ova parasites, Clostridium difficile infection. • Radiographic examination.
Upper gastrointestinal series and small bowel series. • Before test: • -maintain NPO for 8 hr • -withhold analgesics and anticholinergics for 24 hr. • Client drinks 16 ounces of barium. • Rotate examination table. • After the test: • -give plenty of fluids • -administer mild laxative or stool softener; stools may be chalky white for 24 to 72 hr.
Barium Enema • Barium enema enchances radiographic visualization of the large intestine. • Only clear liquids are given 12 to 24 hr before the test; NPO the night before; bowel cleansing is done. • After the test,expel the barium:drink plenty of fluids; stool is chalky white for 24 to 72 hr.
Percutaneous Transhepatic Cholangiography • X-ray study of the biliary duct system • Laxative before the procedure • NPO for 12 hr before test • Coagulation tests, intravenous infusion • Bedrest for several hours after procedure • Assessment of vital signs (Continued)
Percutaneous Transhepatic Cholangiography(Continued) • Client positioned on right side with a firm pillow or sandbag placed against the lower ribs and abdomen
Other Tests • Computed tomography • Endoscopy: direct visualization of the gastrointestinal tract by means of a flexible fiberoptic endoscope
Esophagogastroduodenoscopy • Visual examination of the esophagus, stomach, and duodenum • NPO for 6 to 8 hr before the procedure • Conscious sedation • After the test, assessment of vital signs every 30 min • NPO until gag reflex returns • Throat discomfort possible for several days
Endoscopic RetrogradeCholangiopancreatography • Visual and radiographic examination of the liver, gallbladder, bile ducts, and pancreas • NPO for 6 to 8 hr before test • Access for intravenous sedation • After the test, assessment of vital signs every 15 min (Continued)
Endoscopic Retrograde Cholangiopancreatography(Continued) • Return of gag reflex checked • Assessment for pain • Colicky abdominal pain
Small Bowel Capsule Enteroscopy • Visualization of the small intestine • Only water for 8 to 10 hr before test • NPO for first 2 hr of the testing • Application of belt with sensors
Colonoscopy • Endoscopic examination of the entire large bowel • Liquid diet for 12 to 24 hr before procedure, NPO for 6 to 8 hr before procedure • Bowel cleansing routine • Assessment of vital signs every 15 min • If polypectomy or tissue biopsy, blood possible in stool
Proctosigmoidoscopy • Endoscopic examination of the rectum and sigmoid colon • Liquid diet 24 hr before procedure • Cleansing enema, laxative • Position client on left side in the knee-chest posture. (Continued)
Proctosigmoidoscopy(Continued) • Mild gas pain and flatulence from air instilled into the rectum during the examination • If biopsy was done, a small amount of bleeding possible
Gastric Analysis • Measurement of the hydrochloric acid and pepsin content for evaluation of aggressive gastric and duodenal disorders (Zollinger-Ellison syndrome) • Basal gastric secretion and gastric acid stimulation test • NPO for 12 hr before test • Nasogastric tube insertion
Other Tests • Ultrasonography • Endoscopic ultrasonography • Liver-spleen scan