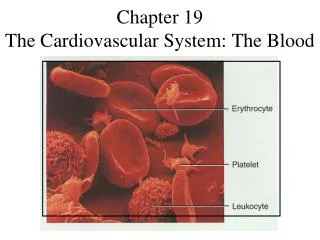
Download
1 / 54
620 likes | 1.56k Vues
Marieb Chapter 19 Part A: Blood Vessels. Arterial system. Venous system. Large veins (capacitance vessels). Heart. Elastic arteries (conducting vessels). Large lymphatic vessels. Lymph node. Muscular arteries (distributing vessels). Lymphatic system. Small veins (capacitance

E N D
Arterial system Venous system Large veins (capacitance vessels) Heart Elastic arteries (conducting vessels) Large lymphatic vessels Lymph node Muscular arteries (distributing vessels) Lymphatic system Small veins (capacitance vessels) Arteriovenous anastomosis Lymphatic capillary Sinusoid Arterioles (resistance vessels) Postcapillary venule Terminal arteriole Metarteriole Thoroughfare channel Precapillary sphincter Capillaries (exchange vessels) Figure 19.2
Tunica intima Valve • Endothelium • Subendothelial layer Internal elastic lamina Tunica media (smooth muscle and elastic fibers) External elastic lamina Tunica externa (collagen fibers) Lumen Vein Lumen Artery Capillary network Basement membrane Endothelial cells Capillary (b) Figure 19.1b
Elastic (Conducting) Arteries • Large thick-walled arteries with elastin in all three tunics • Aorta and its major branches • Large lumen offers low-resistance • Act as pressure reservoirs—expand and recoil as blood is ejected from the heart • The recoil keeps blood flowing when the entire heart is in diastole. • What would happen if recoil couldn’t occur?
Muscular (Distributing) Arteries and Arterioles • Distal to elastic arteries; deliver blood to body organs • Have thick tunica media with more smooth muscle • Arterioles control flow into capillary beds via vasodilation and vasoconstriction
Capillaries • Microscopic blood vessels • Walls of thin tunica intima, one cell thick • Size allows only a single RBC to pass at a time (blood flow slows and RBCs need to flex to get through) • Diffusion of nutrients and wastes
Capillary Beds • Networks of microscopic capillaries link arterioles and venules • Two types of vessels • Vascular shunt (metarteriole — thoroughfare channel): • Directly connects a terminal arteriole and a postcapillary venule • Always remain open so tissue receives oxygen and nutrients 2. True capillaries • 10 to 100 vessels per bed • Branch off the metarteriole or terminal arteriole • Precapillary sphincters can shut off flow
Arterial system Venous system Large veins (capacitance vessels) Heart Elastic arteries (conducting vessels) Large lymphatic vessels Lymph node Muscular arteries (distributing vessels) Lymphatic system Small veins (capacitance vessels) Arteriovenous anastomosis Lymphatic capillary Sinusoid Arterioles (resistance vessels) Postcapillary venule Terminal arteriole Metarteriole Thoroughfare channel Precapillary sphincter Capillaries (exchange vessels) Figure 19.2
Blood Flow Through Capillary Beds • Precapillary sphincters regulate blood flow into true capillaries • Primarily regulated by local chemical conditions ( , and )
Vascular shunt Precapillary sphincters Thoroughfare channel Metarteriole True capillaries Terminal arteriole Postcapillary venule (a) Sphincters open—blood flows through true capillaries. Terminal arteriole Postcapillary venule (b) Sphincters closed—blood flows through metarteriole thoroughfare channel and bypasses true capillaries. Figure 19.4
Veins • Formed when venules converge • Have thinner walls, larger lumens than arteries • Blood pressure is much lower than in arteries • Called capacitance vessels (blood reservoirs); contain up to ______ of the blood supply • Veins stretch (like ) • In what body regions do they stretch and why?
Vein Artery (a) Figure 19.1a
Where is the blood, at rest? Pulmonary blood vessels 12% Systemic arteries and arterioles 15% Heart 8% Capillaries 5% Systemic veins and venules 60% Figure 19.5
Physiology of Circulation: Definition of Terms • Blood flow • Volume of blood flowing through a vessel, an organ, or the entire circulation in a given period • Measured as ml/min or L/min • Equivalent to cardiac output (CO) for entire vascular system • Relatively constant when at rest • Varies widely through individual organs, based on needs
Physiology of Circulation: Definition of Terms • Blood pressure (BP) • Force per unit area exerted on the wall of a blood vessel by the blood • Expressed in mm Hg (systolic/diastolic) • Can calculate an average value (MAP) • Measured as systemic arterial BP in large arteries near the heart • A pressure gradient keeps blood moving from higher to lower pressure areas
Physiology of Circulation: Definition of Terms • Resistance (peripheral resistance) • Opposition to flow • Measure of the amount of friction the blood encounters • Mostly in the peripheral systemic circulation • Three important sources of resistance: • Blood viscosity • Total blood vessel length • Blood vessel diameter
Resistance • Factors that remain relatively constant: • Blood viscosity • The “stickiness” of the blood due to formed elements and plasma proteins remember the karo syrup? • Blood vessel length • The longer the vessel, the greater the resistance encountered • Need more pressure to send water through a longer hose!
Resistance • Changing vessel diameter significantly alters peripheral resistance • Varies inversely with the fourth power of vessel radius • E.g., if the radius is doubled, the resistance is 1/16 as much (not 1/2 as you would expect)
Resistance • Small-diameter arterioles are the site of change in peripheral resistance • Abrupt changes in diameter or fatty plaques from atherosclerosis dramatically increase resistance • Disrupt laminar flow and cause turbulence
Relationship Between Blood Flow and Resistance • Blood flow is inversely proportional to peripheral resistance (R) • If R increases, blood flow decreases • R is more important in influencing local blood flow because it is easily changed by altering blood vessel diameter
Systemic Blood Pressure • The pumping action of the heart generates blood flow • Pressure results when the flow is opposed by resistance • Systemic pressure is highest in the aorta and then declines throughout the pathway • The steepest drop occurs in arterioles
Systolic pressure Mean pressure Diastolic pressure Figure 19.6
Arterial Blood Pressure • Systolic pressure: pressure exerted during ventricular contraction • Diastolic pressure: lowest arterial pressure when the heart is completely at rest
Arterial Blood Pressure • Mean arterial pressure (MAP): average pressure that propels the blood to the tissues MAP = diastolic pressure + 1/3 (Systolic - diastolic) • MAP declines with increasing distance from the heart
Let’s Calculate Some MAP Values • BP is 115/85 • BP is 145/95 • BP is 105/60
Capillary Blood Pressure • Ranges from only 15 to 35 mm Hg • Low capillary pressure is desirable • High BP would rupture fragile, thin-walled capillaries • Most are very permeable, so low pressure forces filtrate into interstitial spaces
Maintaining Blood Pressure • Requires the heart, blood vessels, and kidneys to work together • Supervision by the brain
Maintaining Blood Pressure • The main factors influencing blood pressure: • Cardiac output (CO) • Peripheral resistance (TPR) • Blood volume (BV)
Maintaining Blood Pressure • Blood pressure = CO x PR (and CO depends on blood volume) • MAP = CO X TPR = (SV X HR) X TPR • Blood pressure varies directly with CO, TPR, and blood volume • Changes in one variable are quickly compensated for by changes in the other variables
Cardiac Output (CO) • Determined by venous return and neural and hormonal controls • Resting heart rate is maintained by the CIC via the parasympathetic vagus nerves • Stroke volume is controlled by preload (EDV)
Cardiac Output (CO) • During stress, the CAC increases heart rate and stroke volume via sympathetic stimulation • ESV decreases and MAP increases
Exercise BP activates cardiac centers in medulla Parasympathetic activity Activity of respiratory pump (ventral body cavity pressure) Sympathetic activity Activity of muscular pump (skeletal muscles) Epinephrine in blood Sympathetic venoconstriction Venous return Contractility of cardiac muscle EDV ESV Stroke volume (SV) Heart rate (HR) Initial stimulus Physiological response Cardiac output (CO = SV x HR Result Figure 19.8
Control of Blood Pressure • Short-term neural and hormonal controls • Oppose blood pressure changes by altering peripheral resistance (VMC action) • Also regulate HR and force of contraction • Long-term renal regulation • Counteracts fluctuations in blood pressure by altering blood volume (renin-angiotensin)
Short-Term Mechanisms: Neural Controls • Neural controls operate via reflex arcs that use: • Baroreceptors • Vasomotor centers and vasomotor fibers • Vascular smooth muscle
The Vasomotor Center • A cluster of sympathetic neurons in the medulla that send a message to change blood vessel diameter • Part of the cardiovascular center, along with the cardiac centers • Maintains vasomotor tone (moderate constriction of arterioles by symp NS) • Receives inputs from baroreceptors, chemoreceptors, and higher brain centers
Short-Term Mechanisms: Baroreceptor-Initiated Reflexes • Baroreceptors are located in the: • Carotid sinuses • Aortic arch • Walls of large arteries of the neck and thorax
Short-Term Mechanisms: Baroreceptor-Initiated Reflexes • Increased blood pressure stretches the baroreceptors so they fire faster • Inhibits the vasomotor center (VMC), causing arteriole dilation and venodilation • Inhibits the cardioacceleratory center (CAC) • Stimulates the cardioinhibitory center (CIC)
3 Impulses from baroreceptors stimulate cardioinhibitory center (and inhibit cardioacceleratory center) and inhibit vasomotor center. 4a Sympathetic impulses to heart cause HR, contractility, and CO. 2 Baroreceptors in carotid sinuses and aortic arch are stimulated. 4b Rate of vasomotor impulses allows vasodilation, causing R 5 CO and R return blood pressure to homeostatic range. 1 Stimulus: Blood pressure (arterial blood pressure rises above normal range). Homeostasis: Blood pressure in normal range 1 Stimulus: Blood pressure (arterial blood pressure falls below normal range). 5 CO and R return blood pressure to homeostatic range. 4b Vasomotor fibers stimulate vasoconstriction, causing R 2 Baroreceptors in carotid sinuses and aortic arch are inhibited. 4a Sympathetic impulses to heart causeHR, contractility, and CO. 3 Impulses from baroreceptors stimulate cardioacceleratory center (and inhibit cardioinhibitory center) and stimulate vasomotor center. Figure 19.9
What happens when the blood pressure rises? 3 Impulses from baroreceptors stimulate cardioinhibitory center (and inhibit cardioacceleratory center) and inhibit vasomotor center. 4a Sympathetic impulses to heart cause HR, contractility, and CO. 2 Baroreceptors in carotid sinuses and aortic arch are stimulated. 4b Rate of vasomotor impulses allows vasodilation, causing R 5 Stimulus: Blood pressure (arterial blood pressure rises above normal range). 1 CO and Rreturn blood pressure to homeostatic range. Homeostasis: Blood pressure in normal range Figure 19.9 step 5
What happens when the blood pressure falls? Homeostasis: Blood pressure in normal range 1 Stimulus: Blood pressure (arterial blood pressure falls below normal range). 5 CO and R return blood pressure to homeostatic range. 4b Vasomotor fibers stimulate vasoconstriction, causing R 2 Baroreceptors in carotid sinuses and aortic arch are inhibited. 4a Sympathetic impulses to heart cause HR, contractility, and CO. 3 Impulses from baroreceptors stimulate cardioacceleratory center (and inhibit cardioinhibitory center) and stimulate vasomotor center. Figure 19.9 step 5
Short-Term Mechanisms: Baroreceptor-Initiated Reflexes • Baroreceptors taking part in the carotid sinus reflex protect the blood supply to the brain • Respond to MAP of 40 - 180 mm Hg • Baroreceptors taking part in the aortic reflex help maintain adequate blood pressure in the systemic circuit • Respond to MAP > 100 mm Hg
Short-Term Mechanisms: Chemoreceptor-Initiated Reflexes • Chemoreceptors are located in the • Carotid sinus • Aortic arch • Large arteries of the neck • Pretty much in the same places as the baroreceptors!
Short-Term Mechanisms: Chemoreceptor-Initiated Reflexes • Chemoreceptors respond to rise in CO2, drop in pH or O2 • Increase blood pressure via the vasomotor center and the cardioacceleratory center • Are MUCH more important in the regulation of respiratory rate and depth (Chapter 22)
Short-Term Mechanisms: Hormonal Controls • Adrenal medulla hormones norepinephrine (NE) and epinephrine cause generalized vasoconstriction and increase cardiac output • Angiotensin II, generated by kidney release of renin, causes vasoconstriction
Short-Term Mechanisms: Hormonal Controls • Atrial natriuretic peptide causes blood volume and blood pressure to decline, causes generalized vasodilation • Antidiuretic hormone (ADH)(vasopressin) causes intense vasoconstriction in cases of extremely low BP
Long-Term Mechanisms: Renal Regulation • Baroreceptors adapt ( ) to chronic high or low BP • Since they stop working, what does our body then do? • Let the kidneys spring into action to regulate arterial blood pressure • Direct renal mechanism via blood volume • Indirect renal (renin-angiotensin) mechanism
Indirect Mechanism Involves Renin-Angiotensin • The renin-angiotensin mechanism • Arterial blood pressure release of renin • Renin production of angiotensin II • Angiotensin II is a potent vasoconstrictor • Angiotensin II aldosterone secretion • Aldosterone renal reabsorption of Na+ and urine formation • Angiotensin II stimulates ADH release