Download
1 / 88
900 likes | 1.38k Vues
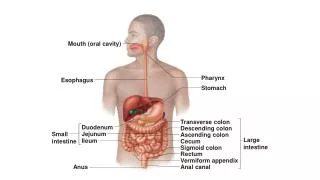
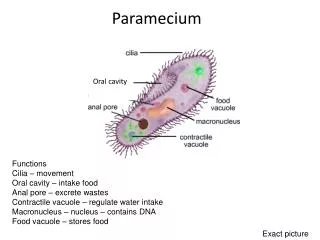
ORAL CAVITY AND OROPHARYNX. Mostafa EL-Haddad Ass. Prof. Of Oncology Kasr Al-Ainy Hospital Cairo University (NEMROCK). Oral Cavity. ANATOMY. Hard Palate. Upper and Lower Gingiva. Lip. Oral Tongue Ant 2/3. Buccal Mucosa. Floor Of mouth. Buccal Mucosa.

E N D
ORAL CAVITY AND OROPHARYNX Mostafa EL-Haddad Ass. Prof. Of Oncology Kasr Al-Ainy Hospital Cairo University (NEMROCK)
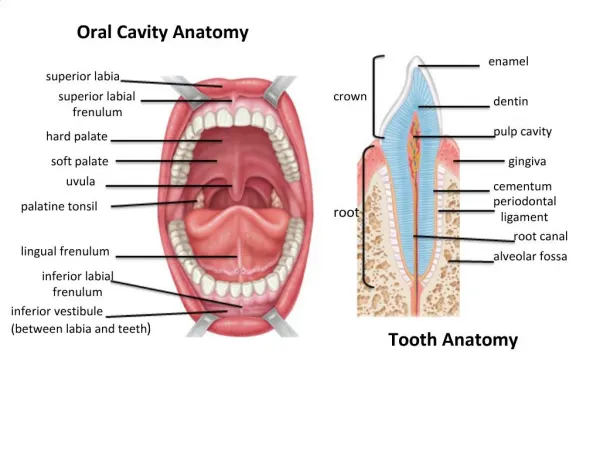
ANATOMY Hard Palate Upper and Lower Gingiva Lip Oral Tongue Ant 2/3 Buccal Mucosa Floor Of mouth Buccal Mucosa Retromolar Trigone or (Retromolar Gingiva
Notes • Retromolar trigone??:-Apex in line with maxillary tuberosity (behind last molar teeth), the lateral border extend with buccal mucosa, medially it blends with anterior tonsillar pillar, base is formed by the last lower molar and the adjacent gingivolingual sulcus.
Other Trigones Trigone of bladder: a triangular region of the wall of the urinary bladder, the three angles corresponding with the orifices of the ureters and urethra; it is an area in which the muscle fibers are closely adherent to the mucosa.
Carotid trigone: the triangular area bounded by the posterior belly of the digastric muscle, the sternocleidomastoid muscle, and the anterior midline of the neck.
Olfactory trigone: The triangular area of gray matter between the roots of the olfactory tract.
Four taste qualities, a novel taste, that is referred by the Japanese word umami which means delicious, ‘‘fifth taste’’. • Umami taste is found in a diversity of foods (e.g. fish, meat, milk, tomato and some vegetables) and is elicited by monosodium glutamate and certain ribonucleotides.
Aging, pregnancy and menopause. Poor dentition and hygiene, alcoholism and/or excessive smoking are common conditions that affect taste. • Patients with xerostomia, Sjogren syndrome, vitamin and zinc deficiency liver and kidney disorders, endocrine disorders, diabetes mellitus, psychological disorders,
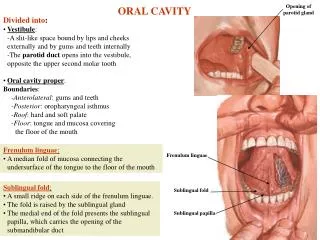
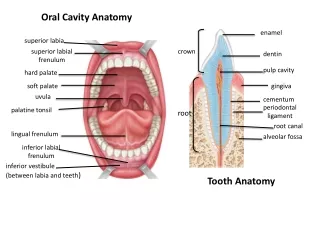
Floor of Mouth • A semilunar space extending from the lower alveolar ridge to the undersurface of the tongue. • The floor of the mouth overlies the mylohyoid and hyoglossus muscles.
Tongue Nerve Supply • Lingual (Meneeein). • Chorada Tympani. • Hypoglossal Nerve.
Staging • As other Head and Neck but not Nasopharynx.
T4a and T4b • Usually T4b tumor control probability is very low. • Resectability is impossible.
Examination Under Anesthesia can be done with the surgeon to assess the disease similar to that of the Cervix.
Start by Support • Nutritional support. • Dental Support. • Psychological Support. • Speech and Swallowing Consult.
The 5-year cancer-specific survival can be as high as 70% to 90% for patients without lymph node metastasis but drops by half for patients with node-positive disease.
Staging and Node in Head and Neck Cancer • N2 disease put patient Stage IVA. • N3 disease put patient Stage IVB.
Nodes N0 • should be treated prophylactically Level I to III.
ORAL CAVITY BASICS • ASK YOUR SELF THREE QUESTION? • Is it small (T1 or T2 ) or large (T3 or T4)?. • Is the lesion Central or Lateralized?. • Is the Nodes negative or Positive?.
Rules • The closer to the midline the primary, the greater the risk of bilateral cervical nodal spread. • The mucosa of the upper and lower alveolus and hard palate is fixed to the underlying periosteum so invasion of the adjacent bone occurs relatively early making these tumors less suitable for primary radiotherapy
Early Lesion • Surgical resection: where rim rather segmental resection should be performed. Situations where removal of the bone is required to achieve clear margin. • Re-resection should be performed to achieve clear histological margins if the initial resection has positive margins.
Lymphatics • incidence of clinical nodal positivity at presentation • according to anatomic subsite: • 20 – 30% for gingival and retromolar trigone tumors (with slightly higher risk of nodal disease for lower gingival vs upper gingival tumors) and 10% for hard palate tumors • - incidence of clinically positive bilateral nodes rare • incidence of occult nodal disease overall: 20%
Planned Neck dissection • What does it mean? • Controversy continue.
In Early stage T1 and T2 surgery results equal to RT. • So How to choose?
LIP • Surgery may be preferred in : - T1 lesion with good functional and cosmetic outcome. - Young patient with outdoor sunlight exposure. - Diffuse superficial lesion of the vermillion, or presence of severe actinic keratosis adjacent to carcinoma.
N0 disease • In the N0 neck, occult metastases are estimated to occur in 5% to 10% of cases. • Therefore, elective neck dissection is not routinely performed in the N0 neck. • Neck dissections are generally performed when cervical metastases are clinically or radiographically apparent.
Primary Radiotherapy • Target Volume: • Tumor with a margin • Tumor with a margin+first echlon lymph nodes. • Tumor with a margin + whole neck . WHEN?
LIP What is the likely diagnosis? How would you treat this patient (describe your technique in detail)
Tumor Thickness in Oral Tongue • Po demonstrated that tumor thickness in oral tongue carcinomas was the only significant factor that had significant predictive value for subclinical nodal metastasis, local recurrence, and survival in multivariate analysis.
External beam alone may not be very successful. • Boost using brachytherapy is recommended.