Download
1 / 8
80 likes | 343 Vues
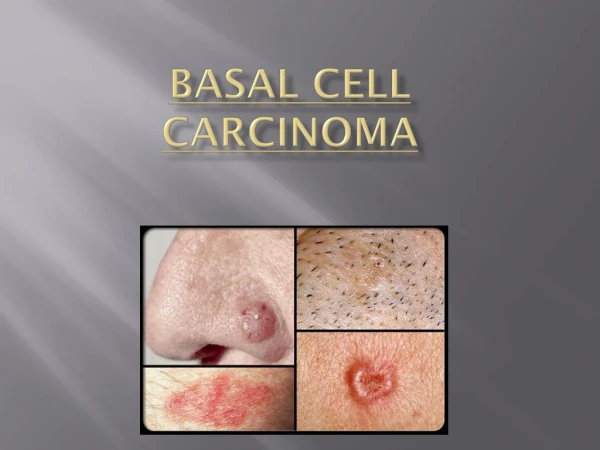
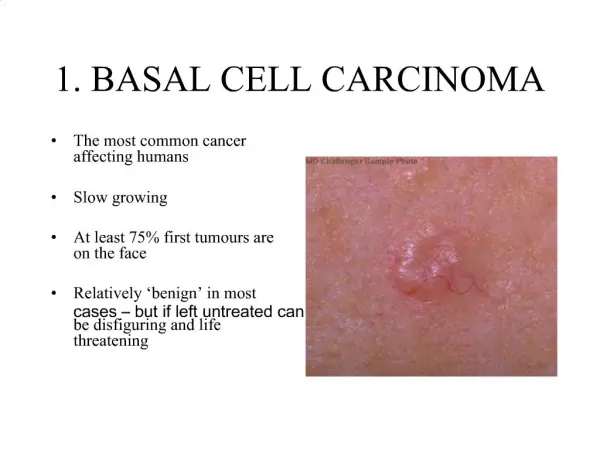
Describe the clinical features of skin cancers and the features that may differentiate between squamous cell carcinoma, basal cell carcinoma and melanoma. Basal Cell Carcinoma (rodent ulcer) Most common malignant skin tumor and primarily related to chronic sun exposure.

E N D
Describe the clinical features of skin cancers and the features that may differentiate between squamous cell carcinoma, basal cell carcinoma and melanoma
Basal Cell Carcinoma (rodent ulcer) • Most common malignant skin tumor and primarily related to chronic sun exposure. • Occur mostly in elderly on exposed sites → Common on the face, less common on ear. • Present as slow growing papule or nodule (rarely cystic) which may ulcerate (common). • Often have tiny blood vessels visible on border (telangiectasia) and/or raised 'pearly' jelly-like edge. • Contains cells similar in appearance to normal basal layer of epidermis and are believed to arise from this layer and hair follicles. • May be highly invasive and locally destructive but rarely metastasise. • Local excision depends on whether the BCC is: → low risk (nodular) → high risk (superficial or morphoeic/infiltrative)
Squamous Cell Carcinoma • More aggressive than BCC and can metastasise if untreated. • Most relate to sun exposure but can arise in pre-existing solar keratoses (pre-malignant dysplasia), Bowen's disease or from chronic inflammation. → common on sun exposed sites in elderly • Multiple tumors rarely occur due to arsenic ingestion when young or more commonly in long periods of immunosupression. • Lesions are often rough, keratotic, ill defined nodules which may have ulcers of horns. → lower lip or ear lesions highly suspicious. • Grow rapidly, require examination of regional lymph nodes. • Composed of disorganised keratinocytes with malignant cytology.
Malignant Melanoma • Most serious form as metastases can occur early and in young people. • Risks include: Hx of childhood and intermittent sun exposure, atypical mole syndrome, giant congenital melanocytic naevi, lentigo maligna and a +ve family Hx of melanoma. • Sites include legs in young women, back in young men and face in elderly. • Melanin pigment visible in cells with nuclear pleomorphism. • 4 clinical types: • 1) Lentigo maligna melanoma – patch of lentigo maligna develops into papule or nodule in elderly → invasion. • 2) Superficial spreading malignant melanoma – large, flat, irregularly pigmented lesion which grows laterally before vertical invasion. • 3) Nodular malignant melanoma – Most agressive. Rapidly growing, pigmented nodule which bleeds/ulcerates. Typically pigmented. • 4) Acral lentiginous malignant melanoma – Pigmented lesions on palm, sole or under nail. Late presentation.
Clinical Criteria for Dx • ABCDE Criteria • Asymmetry of mole • Border irregularity • Colour variegation • Diameter > 6mm • Elevation • Glasglow 7-point Checklist • Major criteria • → change in size • → change in shape • → change in colour • Minor criteria → diameter > 6mm → inflammation → oozing or bleeding → Mild itch or altered sensation