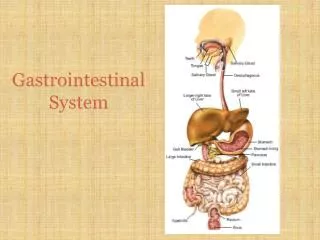
Conditions of the Gastrointestinal System
Conditions of the Gastrointestinal System Part A: Module A2 Session 5 Objectives Describe the various infectious agents that cause chronic diarrhea Describe the clinical presentation of each infection List the recommended diagnostics and common findings for each infection

Conditions of the Gastrointestinal System
E N D
Presentation Transcript
Conditions of the Gastrointestinal System Part A: Module A2 Session 5
Objectives • Describe the various infectious agents that cause chronic diarrhea • Describe the clinical presentation of each infection • List the recommended diagnostics and common findings for each infection • Understand the treatment and management of chronic diarrhea • Discuss hepatitis, including management, treatment, and prevention • Make a differential diagnosis using a case study approach
Overview • Chronic diarrhea is a very frequent and frustrating problem in PLHA: at least 50% experience it sometime during the evolution of the disease • Often accompanied by nausea, weight loss, abdominal cramps, and dehydration • Often an intermittent watery diarrhea, without blood or mucous • In one-third to two-thirds of cases, no cause is identified • In high HIV prevalence areas, chronic diarrhea is invariably due to symptomatic HIV infection.
Wherever possible the cause should be established and specific treatment given • If cause is not established, management is symptomatic: giving anti-diarrheals such as codeine phosphate • The key to good management is rehydration without much sugar, and including potassium • High energy and protein intake reduces the degree of muscle wasting • Prevention consists of: attention to personal hygiene (hand-washing), drinking boiled water, and eating only thoroughly cooked meat and vegetables
Major Pathogens Bacterial infectionCampylobacter, Shigella, and Salmonella Protozoal infection Cryptosporidium species, Giardia lamblia, Isospora belli, Entamoeba histolitica, Microsporidium species Toxin induced E. coli and Clostridium difficile Mycobacterial infection M. tuberculosis, M. Avium complex Helminthic infection Strongyloides stercoralis Fungal infection Candida species (seldom a cause of diarrhea)
Chart 3. Conditions of the Gastrointestinal System: Chronic Diarrhea
Bacterial infection: Campylobacter Presenting Signs and Symptoms • Clinical Symptoms may evolve • Fever and general malaise, sometimes without GI symptoms • When present, GI symptoms include bloody diarrhea, abdominal pain and weight loss.
Campylobacter: Diagnostics • Campylobacter bacilli found in stool culture
Campylobacter Management and Treatment • Erythromycin 500 mg bid x 5 days (1st choice) • Fluoroquinolones are also effective, but resistance rates of 30-50% have been reported in some developing countries
CampylobacterUnique features, Caveats • It is clinically impossible to distinguish the different etiological agents of bacterial gastroenteritis without a stool culture • If empiric therapy with TMP/SMX is not effective in patients with bacillary dysentery, try fluoroquinolones • If symptoms of bloody diarrhea persist , try erythromycin
Bacterial infection: Salmonella Presenting Signs and Symptoms • Clinical Symptoms may evolve • Fever; general malaise • Sometimes no GI symptoms • If there are GI symptoms, will see: • Bloody diarrhea • Abdominal pain • Weight loss
Bacterial infection: SalmonellaDiagnostics • Stool culture • Salmonella bacilli may be found in stool/blood cultures • Serology: positive Widal test with increased titers
Management and Treatment • TMP/SMX 960 mg bid or • Chloramphenicol 250 mg qid for 3 weeks • In case of sepsis, IV therapy is necessary • Shorter regimens are: • ciprofloxacin 500 mg bid or ofloxacin 400 mg bid or ceftriaxone 2 g IV for 7-10 days • Many patients often relapse after treatment and chronic maintenance therapy (TMP/SMX 1 DD daily) is sometimes necessary.
Unique features, Caveats • Salmonellosis is a frequent cause of bacteremia in PLHA
Bacterial infection: Shigella Presenting Signs and Symptoms • Clinical Symptoms may evolve • High fever • Abdominal pain • Bloody diarrhea
ShigellaDiagnostics • Stool microscopy— fresh examination and after concentration • Multiple stool samples may be necessary • Shigella bacillus found in stool
ShigellaManagement and Treatment • TMP/SMX 960 mg bid x 5 days or • amoxicillin 500 mg tid x 5 days • If resistant to the above, give • ciprofloxacin 500 mg bid • or • norfloxacin 400 mg bid x 5 days • or • nalidixic acid 1 g qid x 10 days
Unique features, Caveats In many developing countries resistance of Shigella (and Salmonella) to TMP/SMX has increased.
Protozoal infection: Clostridium difficile Presenting Signs and Symptoms • Clinical Symptoms may evolve • Diarrhea • Fever
Clostridium difficileDiagnostics • Stool microscopy and culture
Clostridium difficileUnique features, caveats • May be underestimated as a cause of diarrhea in AIDS patients in the tropics because of the difficulty in making the diagnosis. Frequent hospitalization and exposure to antibiotics puts patients at high risk of infection • As in HIV-negative patients, 5-30% of patients with C. difficile-associated diarrhea experience relapse
Protozoal infection: Cryptosporidium Presenting Signs and Symptoms • Clinical Symptoms may evolve • Recent and prolonged history of severe diarrhea—usually large volume, watery stools with a lot of abdominal pain, bowel noise and activity • Severe weight loss/wasting in those with longer history
Cryptosporidium Diagnostics • Stool samples x 3 for staining/AFB smear • Oocysts present in stool exam • No fecal WBCs
Cryptosporidium Management and Treatment • Rehydration (IV and/or ORS) • Paromomycin 500 mg qid for 2-3 weeks; maintenance with 500 mg bid often required • Codeine phosphate 30-60 mg tid until under control (or other anti-diarrheal agents such as loperamide 2-4 mg tid or qid—maximum of 32 mg in 24 hours) • The use of ARV is protective against cryptosporidiosis
Cryptosporidium Unique features, Caveats • Highly infectious • Transmitted through water, food, animal-to-human and human-to-human contact • Special precautions should be taken to prevent exposure: people with HIV and a CD4<200 should boil tap water for at least 1 minute to reduce risk of ingestion of oocysts in potentially contaminated drinking water. • May be the AIDS-defining presentation in patients who previously had few symptoms of HIV infection
Toxin induced: E. coli Presenting Signs and Symptoms • Clinical Symptoms may evolve • Diarrhea • Fever
Toxin induced: E. coli Diagnostics • Stool microscopy and culture
Entamoeba histolytica Presenting Signs and Symptoms • Clinical Symptoms may evolve • Colitis • Bloody stools • Cramps • Can be asymptomatic
Entamoeba histolytica Diagnostics • Stool for ova and parasite exam • O&P present in stool exam • No fecal WBC’s
Entamoeba histolyticaManagement and Treatment • metronidazole 500-700 mg po or IV tid x 5-10 days or • paromomycin 500 mg po qid x 7 days
Entamoeba histolytica Unique features, Caveats • E. histolytica may be common in the general population in developing countries, but may be recurrent or more severe in HIV patients
Giardia lamblia Presenting Signs and Symptoms • Clinical Symptoms may evolve • Enteritis • Watery diarrhea malabsorption • Bloating • Flatulence
Giardia lamblia Diagnostics • Stool for ova and parasites • O&P in stool exam
Giardia lamblia Management and Treatment • Metronidazole 250 mg po tid x 10 days
Giardia lamblia Unique features, Caveats • Common cause of diarrhea in general population, but may be recurrent or more severe in HIV patients
Isospora belli Presenting Signs and Symptoms • Clinical Symptoms may evolve • Enteritis; watery diarrhea • No fever • Wasting; malabsorption ** Symptoms similar to what occurs with Cryptosporidium
Giardia lambliaDiagnostics • Stool x 3: unstained wet preparation • Isospora belli oocysts are relatively big (2030 m) and can be easily identified in unstained wet stool preparation • No fecal WBCs
Giardia lamblia Management and Treatment • Most cases are readily treated with sulfamethoxazole/ trimethoprim (960 mg qid for 10 days) followed by 1 double strength tablet (960 mg bid for 3 weeks), then chronic suppression with sulfamethoxazole/ trimethoprim (960mg daily) • High dose of pyrimethamine with calcium folinate to prevent myelosuppression • Long-term maintenance therapy may be required to prevent relapse
Microsporidium Presenting Signs and Symptoms • Clinical Symptoms may evolve • Profuse watery, non-bloody diarrhea • Abdominal pain and cramping • Nausea • Vomiting • Weight loss
Giardia lambliaDiagnostics • Fresh stool microscopy with modified trichrome stain • Spores present in stool exam
Giardia lambliaUnique features, Caveats • Species of microsporidia have been linked to disseminated disease, e.g., cholangitis, keratoconjunctivitis, hepatitis, peritonitis, and infections of the lungs, muscles, and brain • However, the presence of microsporidia does not always correlate with symptomatic disease • Most microsporidial infections are not treatable
Helminthic infection: Strongyloides stercoralis Presenting Signs and Symptoms • Clinical Symptoms may evolve • Serpiginous erythematous skin lesions (larva currens) • Diarrhea • Abdominal pain • Cough • Full-blown hyper-infection syndrome has the characteristics of a gram-negative sepsis, with acute respiratory distress syndrome, disseminated intravascular coagulation, and secondary peritonitis, cough
Strongyloides stercoralisDiagnostics • Chest x-ray: The chest x-ray may reveal diffuse pulmonary infiltrates. • Stool microscopy, (multiple stool samples may be necessary) • Sputum sample • In disseminated strongyloidiasis, filariform larvae can be found in stool, sputum, broncho-alveolar lavage fluid, pleural fluid, peritoneal fluid and surgical drainage fluid
Strongyloides stercoralisManagement and Treatment • Ivermectin 12 mg daily for 3 days. This drug is also the drug of choice for the treatment of systemic strongyloidiasis • An alternative treatment is albendazole 400 mg bid x 5 days • A maintenance therapy once a month is necessary to suppress symptomatic infection (albendazole 400 mg or ivermectin 6 mg once monthly)
Strongyloides stercoralisUnique features, Caveats • In immuno-compromised patients, strongyloides can cause overwhelming infection.This serious complication is called strongyloides hyper-infection syndrome and has a high case-fatality rate • Disseminated strongyloidiasis and heavy worm loads can occur in patients with HIV, but the full-blown hyper-infection syndrome is less common • The likelihood of developing the hyper-infection syndrome is also increased in patients taking high-dose steroids
Other: Hepatitis Presenting Signs and Symptoms • Clinical Symptoms may evolve • Flu-like symptoms of lassitude, weakness, drowsiness, anorexia, nausea, abdominal discomfort, fever, headache, jaundice (including dark urine, gray stools, and mild pruritis), • Hepatomegaly
HepatitisManagement and Treatment • Symptomatic and supportive care. Where available, Interferon for treatment of Hepatitis B and C and Havrix as a preventive measure for patients at risk for hepatitis A; Interferon for treatment of Hepatitis B and C. Epivir-HBV for Hep B • Alcohol consumption should be discouraged during convalescence
HepatitisPrevention • Frequent hand-washing and good hygiene are important as Hepatitis A is spread by oral-fecal route and often by food contamination • Hepatitis B and C are transmitted through contact with blood or through sexual contact • Condoms can reduce risk of transmission • It is important to discourage needle sharing