Download
1 / 1
80 likes | 374 Vues
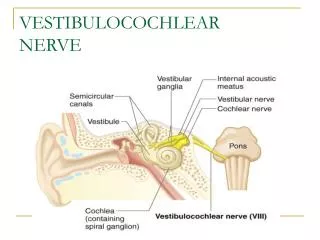
&. Oakdale. ear, nose & throat. Clinic. Dichotic Interaural Intensity Difference (DIID) Training: Auditory Remediation after CVA Annette Hurley, Ph.D. 1 & Cassandra Billiet, Au.D. 2 School of Allied Health Professions, Louisiana State University Health Sciences Center - New Orleans, LA

E N D
& Oakdale ear, nose & throat Clinic Dichotic Interaural Intensity Difference (DIID) Training: Auditory Remediation after CVA Annette Hurley, Ph.D.1 & Cassandra Billiet, Au.D.2 School of Allied Health Professions, Louisiana State University Health Sciences Center - New Orleans, LA Oakdale Ear, Nose, & Throat - Maple Grove, MN During the training period, numerous stimuli were used such as Single and Double Pair Dichotic Digits, Synthetic Sentence Identification, Competing Sentences, Dichotic CVs, the Competing Words and Competing Sentences subtests of the SCAN-A, and Time Compressed Speech. After ten training sessions, binaural separation abilities for the right ear pathway improved from 0% to scores that were within normal limits (>90%). However, binaural integration and auditory closure abilities although improved, remained impaired. Post training electrophysiological recordings showed an increase in the Na-Pa amplitude of the MLR for all electrode sites when stimulating the left ear. No differences in the P300 recordings were noted. Figure 1. Electrophysiological Recordings for Case 1. Figure 1A shows pre and post differences in wave V latency for the right and left ears. Figures 1b show an enhancement of the Na/Pa wave post training for the left ear. Amplitudes are listed for each electrode are listed in the table below. A. B. Perceptual differences in hearing were reported by the patient. During training sessions, the patient reported that the time arrival of the dichotic signals was closer together in time, and that he recognized the signals were at the same time. He initially heard the signal in the left ear first; later the signal from the right ear arrived first. He also reported that he recognized that the speaker was the same in both ears. Previously, he thought there were two distinct voices. These comments substantiate our findings of auditory plasticity or the ability to improve central auditory function through auditory training. Informal auditory training continues. A 46 year old male who was referred for a (C)APD assessment 24 months post CVA. An MRI revealed a large left frontal lobe lesion extending to the parietal lobe. The patient has participated in speech therapy since the time of the CVA. Communication is very difficult as he suffers from aphasia, apraxia, and dense right hemi-paresis which impairs his ability to write. Pure tone hearing thresholds are within normal limits. Due to the communicative ability of the patient, a limited (C)APD assessment was conducted indicating normal gap detection thresholds and a right ear deficit for dichotic digits. Electrophysiological recordings indicated an ear effect for the MLR with decreased amplitudes for the left ear (the side of the head over the lesion). Dichotic Interaural Intensity Difference Training was initiated to improve auditory comprehension. Because of the patient’s limited communication ability, training stimuli were limited to digits. A communication board was employed so that the subject could point to the correct response. After eight training sessions, binaural separation abilities for the right ear pathway improved from 0% to scores within the 80% range. Post training electrophysiological recordings showed an improvement in the ABR recording and a decrease in wave Pa latency. No differences in the P300 recording were noted. Figure 2. Electrophysiological Recordings for Case 2. A slight decrease in wave V latency for the right and left ears is shown in the ABR tracing below. Figure B shows a very slight change in wave Pa latency. A. B. Subjectively, this patient’s wife reports that she can speak to him without looking at him and he can understand. She also reports the volume of the television has decreased dramatically. The patient also reports subjective improvement. Auditory training is still ongoing. This investigation holds great clinical significance for persons with aphasia. The inability to understand conversation, follow a television program, or grasp important instructions excludes people with aphasia from daily life activities that insure safety, lend meaning, and improve their quality of life. Currently, auditory therapy/training is not typically used in rehabilitation programs. Dichotic Interaural Intensity Training has the potential to reduce disabling auditory processing impairments in this population. INTRODUCTION Auditory complaints are common in patients who have suffered a cerebral vascular accident (CVA). These complaints may not be investigated, as they are often thought of as natural repercussions of a CVA. A common complaint among these patients is difficulty understanding speech in the presence of background noise. Although a peripheral hearing exam is important, it may not be sufficient for these patients. A (Central) Auditory Processing evaluation provides insight regarding central auditory nervous system function and identifies specific processes that may be deficient. Auditory rehabilitation/training programs can be designed to target specific processes and may remediate the patient’s auditory complaints. This report details the auditory training program for two patients who have suffered a CVA. Specifically, the auditory training components of each program and the behavioral and electrophysiological measures that were used to assess the efficacy of the auditory training program are discussed. A 48 year old male was referred for a (C)APD assessment four months post CVA. An MRI revealed a large subacute infarct in the left temporoparietal area. He presented with difficulty understanding speech, especially in background noise, and a noticeable change in music perception. Normal peripheral hearing was established. The (C)APD assessment indicated decreased dichotic scores for the right auditory pathway due to the anatomical pathway contralateral to the lesion. An abnormal score for time compressed speech stimuli for the right ear was recorded but not for the left ear. Electrophysiological recordings indicated an abnormal auditory brainstem response (ABR) recording for the left ear. A four channel middle latency response (MLR) recording revealed an ear effect with decreased amplitudes for the left ear (the side of the head over the lesion). Dichotic interaural intensity training was initiated. During this training, the target signal for the right ear remained at a constant level (60 dBHL) while the intensity in the opposite ear (left ear) was introduced at a very low level initially and slowly increased over time until the intensity was at equal levels. CASE I • CONCLUSION CLINICAL SIGNIFICANCE CASE II