Download
1 / 17
260 likes | 981 Vues
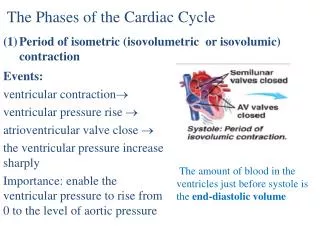
The Phases of the Cardiac Cycle Period of isometric ( isovolumetric or isovolumic ) contraction. Events: ventricular contraction ventricular pressure rise atrioventricular valve close the ventricular pressure increase sharply

E N D
The Phases of the Cardiac Cycle • Period of isometric (isovolumetric or isovolumic) contraction Events: ventricular contraction ventricular pressure rise atrioventricular valve close the ventricular pressure increase sharply Importance: enable the ventricular pressure to rise from 0 to the level of aortic pressure The amount of blood in the ventricles just before systole is the end-diastolic volume
(2)Period of ejection • Events: ventricular contraction continuously • the ventricular pressure rise above the arterial pressure • semilumar valves open blood pours out of the ventricles
Rapid ejection period ( 60% of the stroke volume) • Reduced ejection period (40% of the stroke volume)
(3) Period of isometric (isovolumic) relaxation • Events: • ventricular muscle relax • the ventricular pressure fall • lower than the aortic pressure • aortic valve close • the ventricular pressure fall sharply Importance: Enable the ventricular pressure fall to the level near the atrial pressure
(4) Period of filling of the ventricles Events: Ventricular muscle relax continuously the ventricular pressure is equal or lower than the atrial pressure atrioventricular valve open blood accumulated in the atria rushes into the ventricular chambers quickly from the atrium to the ventricle.
Period of rapid filling. (amount of filling, 2/3) • Period of reduced filling (little blood fills into the ventricle)
(5) Atrial systole • Significance, 30% of the filling • Becomes important in determining the final cardiac output during high output states or in the failing heart
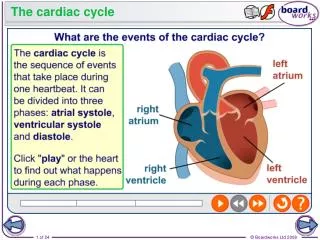
CARDIAC CYCLE Rapid Ventricular Filling Reduced Ejection Rapid Ejection Atrial Systole Isovolumic Relax. Reduced Ventricular Filling Atrial Systole Isovolumic contract. Aortic opens Aortic closes Mitral opens Mitral Closes S1 S2
The Atrial and Central Venous Pressure (CVP) waves • Since there are no valves between the jugular veins (JV), v. cavae ant the RA, the right JV are communicated with the RA. • Changes in pressure in the RA produces a series of pressure changes which are reflected in the central veins and recorded from the JV: a, c and v waves. • CVP is the pressure in the vein at the entrance of the RA • a wave is due to increase in pressure caused by atrial systole • av descent (minimum) is due to relaxation of the right atrium and closure of the tricuspid valve • c wave is caused in the RA by the tricuspid valve bulging back into the atrial chamber as it closes. In the internal JV the c wave (c = carotid) is caused partly by expansions of the carotid artery
X descent is a sharp fall in the pressure caused by atrial relaxation • v wave. As the atria fill, A pressure rises producing v wave (v = ventricular systole which is occurring at the same time) • Y descent is a fall in pressure due to the rapid emptying of the atria after the AV valve opens Fig. 13. Jugular venous pressure changes caused by cardiac cycle
Clinical examination of the JVP • JP of the internal jugular vein can be assessed by expecting the right side of the neck of a recumbent subject. Two sudden venous collapses (the X and Y descent) should be seen and measured externally on the right side of the neck- positive JVP • Certain cardiac diseases produce characteristic abnormalities in the JVP, e.g. tricuspid incompetence produces exaggerated v waves in the neck, because V systole forces blood back into the RA & JV • In right-side cardiac failure there is also a positive JVP due to accumulation of blood into the failing RV and RA
Heart Sounds. The common heart sound are: • The first heart sound is due to the closing of the AV valves • The second heart sound is due to the closing of the aortic and pulmonary valves
Location of the sounds on the chest Each valve is best heard by a stethoscope from 4 distinct areas: Mitral valve: Mid clavicular line of the 5th left intercostal space Tricuspid valve: 5th interspace at the left sternal edge Aortic valve: 2ndinterspace at the right sternal edge Pulmonary valve: 2nd interspace at the left sternal edge
Heart Murmurs: Abnormal heart sounds heard on auscultation which are due to faulty valves. • Incompetence: Failure of the valve to seal properly (valve may be torn, perforated, affected by rheumatic fever or a failing heart may be enlarged) such that it becomes leaky allowing blood to regurgitate through it • Stenosis: The open valve is narrowed so that a higher pressure gradient is needed to drive blood through (cicatrization after rheumatic or other infection) • Defective valves can be congenital or acquired. Abnormal valve causes blood turbulence which sets up high frequency vibrations which are heard as murmurs through the stetoscope
Heart Murmurs (cont.) • Benign Systolic Murmur is common in the young. Caused by turbulence in the ventricular outflow tract. Also during pregnancy, strenuous exercise and anemia • Aortic stenosis: Systolic murmur. Due to narrowing of the aortic valve when the flow during ejection becomes turbulent. Heard during ejection (systolic murmur) as ejection waxes and wanes (a crescendo – decrescendo murmur). Loudest over aortic area • Mitral incompetence: Pan systolic murmur. During V systole blood regurgitates through the mitral valve back into LA resulting a murmur that extends throughout ventricular contraction
Aortic Incompetence: Diastolic murmur When aortic valve does not close completely blood regurgitates back into the V during diastole. The turbulence is upstream of the aortic valve and the murmur begins at the time of S2 and lasts through the early part of diastole. • Mitral Stenosis: Diastolic murmur Blood is forced through the narrowed mitral valve during the phase of ventricular filling – ventricular diastole • Listen to these murmurs at various websites e.g. www.med.ucla.edu/wilkes/intro.html