Download
1 / 23
250 likes | 417 Vues
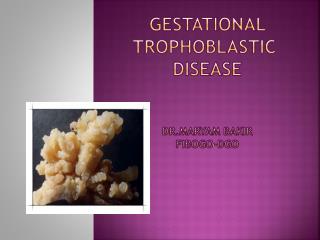
Trophoblastic disease. -This is a group of disorders characterized by 1-abnormal placental development. 2- The chorionic villi are hydropic with vacuolation of the placenta 3- destruction of the normal stroma. Pathology. 1-Benign trophoblastic disease:

E N D
Trophoblastic disease • -This is a group of disorders characterized by • 1-abnormal placental development. • 2- The chorionic villi are hydropic with vacuolation of the placenta • 3- destruction of the normal stroma.
Pathology • 1-Benign trophoblastic disease: • -is usually either a complete hydatidiform mole, where there is no evidence of an embryo, • - or a partial hydatidiform mole which may be associated with an embryo (usually abnormal)
Other types of trophoblastic disease include : • 1-invasive moles • 2-, placental site reactions, • 3- trophoblastictumours and hydropic change.
Malignant trophoblastic disease (choriocarcinoma): • complicates approximately 3% of complete moles although in 50% of cases of choriocarcinoma there is no history of immediately preceding trophoblastic disease.
It may also occur following normal pregnancy. Blood-borne metastases may occur locally in the vagina but most commonly appear in the lungs
Aetiology • Trophoblastic disease is thought to arise by fertilization of the oocyte by a single diploid spermatozoon or by two haploid sperm. • -
If this occurs in the absence of any female nuclear material the resulting conceptus pregnancy is a complete mole with a diploid karyotype (46XX).
-A partial mole is thought to occur where fertilization occurs with the maternal chromosome and the conceptus is triploid (69XXX or 69XXY). • -Older women and those with a previous history of trophoblastic disease or an A type blood group are at increased risk
Presentation • -Molar pregnancy most commonly presents as bleeding in the first half of pregnancy, • - is usually diagnosed initially as a threatened miscarriage. • -Occasionally, the passage of a ‘grape-like’ tissue raises a clinical suspicion • .
- the diagnosis is normally made on ultrasound or after uterine evacuation. • -The uterus is larger than dates in about half the cases. • - Associated conditions include severe hyperemesis, pre-eclampsia and unexplained anaemia and ovarian cysts.
-The high circulating levels of hCG have a TSH like action and can cause clinical thyrotoxicosis. • -Choriocarcinomas may present with the symptoms of distant metastases (cerebral, pulmonary).
Diagnosis • A ‘snowstorm’ appearance with multiple highly reflective echoes and areas of vacuolation within the uterine cavity on ultrasound examination usually suggests molar disease. • - In a partial mole, a gestation sac with a fetus may also be present
- Other imaging, such as chest X-rays, CT or MRI may be indicated to exclude pulmonary or cerebral metastases if choriocarcinoma is suspected. • .
-The diagnosis of trophoblastic disease is confirmed by histological examination of products of conception removed at the time of uterine evacuation
Management • -Once the diagnosis is established, the pregnancy is terminated by suction curettage. • - Occasionally, repeat evacuation may be required if :
1-there is persistent bleeding • 2- or a raised serum hCG but routine second evacuation is not helpful. • - All cases of molar pregnancy in the UK should be registered with one of the trophoblastic disease screening centres who will arrange follow-up.
-The aim of follow-up is to detect persistent trophoblastic disease and choriocarcinoma. • - Because all trophoblastictumours produce hCG patients can be monitored by measurement of urinary or serum hCG levels,
Levels are checked fortnightly until the serum level is <2 IU/L, • - then monthly for 6 months following this if the hCG is negative within 6 weeks of treatment. • - If the hCG takes longer than 6 weeks to become negative, follow-up is continued for a further 12 months
-Patients should be counselled to avoid pregnancy until 6 months after the serum hCG levels fall to normal. • -There is a 0.8–2.9% risk of recurrence in subsequent pregnancies after one mole,
- 15–28% after two moles and serum hCG levels should be checked 6 weeks after any subsequent pregnancy. • -Chemotherapy with methotrexate (with folinic acid rescue) is indicated for a rising hCG level
in the absence of a new pregnancy, an hCG persistently >20 000 IU/L by 4 weeks after treatment, • -persistent symptoms or evidence of metastatic disease. Subsequent fertility does not appear to be
impaired by chemotherapy and there does not seem to be an increased incidence of other chromosomal abnormalities.