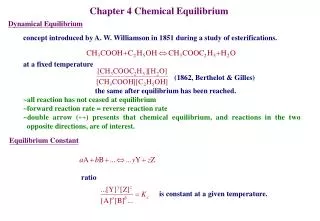
Balance lecture& Postural Equilibrium
Balance lecture& Postural Equilibrium. Dr.Afaf A.M Shaheen lecture 11 RHS 322. Factors affecting balance Muscular weakness Proprioceptive deficits ROM deficits. Terminology. Balance - Process of maintaining body’s CoG (Center of Gravity) within base of support

Balance lecture& Postural Equilibrium
E N D
Presentation Transcript
Balance lecture& Postural Equilibrium Dr.Afaf A.M Shaheenlecture 11RHS 322
Factors affecting balance • Muscular weakness • Proprioceptive deficits • ROM deficits
Terminology • Balance- Process of maintaining body’s CoG (Center of Gravity) within base of support • Ability to align body segments against gravity to maintain or move the body within the available base of support without falling . • Body’s CoG rests slightly above the pelvis • Strength is emphasized before proprioception in rehab because strength influences balance • Postural equilibrium- broader term that incorporates alignment of joint segments • Maintaining CoG within the limits of stability (LOS)
Terminology • Proprioception– body’s ability to transmit position sense, interpret information & respond consciously/unconsciously to stimulation • Coordination – smooth pattern of activity is produced through a combo of muscles acting together with appropriate intensity & timing • Agility – ability to control the direction of a body or segment during rapid movement
Postural Control System • 3 Components of the system • Sensorydetection of body motions • Visual • Vestibular • Somatosensory inputs • Integration of sensorimotor information within the CNS • Execution of musculoskeletal responses • Balance is both a static & dynamic process
Control of Balance • Tall body vs. Small base of support • Balance relies on network of neural connections • Postural control relies on feedback • CNS involvement • Sensory organization • Determines timing, direction & amplitude of correction based on input • System relies on one sense at a time for orientation • Muscle coordination • Collection of processes that determine temporal sequencing & distribution of contractile activity
Sensory Input • Vision • Measures orientation of eyes & head in relation to surrounding objects • Helps maintain balance • Vestibular • Provides information dealing with gravitational, linear & angular accelerations of the head with respect to inertial space • Somatosensory • Provides information concerning relative position of body parts to support surface & each other
Somatosensation = Proprioceptive system • Specialized variation of the sensory modality of touch, encompassing joint sense (kinesthesia) & position • Process • Input from mechanoreceptors • Stretch reflex triggers activation of muscles • Results in muscle response to compensate for imbalance and postural sway • Muscle spindles sense stretch in agonist, relay information afferently to spinal cord • Information is sent back to fire muscle to maintain postural control
Body position in relation to gravity is detected by sensory input • Balance movements involve a number of joints • Ankle • Knee • Hip • Coordinated movement along kinetic chain
Postural sway • Deviation from Center of Pressure, Balance & Vertical Force (CoP, CoB, or CoF) • Determined using mean displacement, length of sway path, length of sway area, amplitude, frequency and direction relative to CoP • Symmetry- Ability to distribute weight evenly between 2 feet in upright stance
Balance Disruption • Balance Deficiencies - Inappropriate interaction among 3 sensory inputs • 2 Factors that Disrupt Balance • Position of CoG relative to base of support is not accurately sensed • Automatic movements required to maintain the CoG are not timely/effective • In the event of contact, the body must be able to determine what to do in order to control CoG • Joint mechanoreceptors initiate automatic postural response
Selecting Movement Strategies during Balance Disruption • Joints (Ankle, Knee & Hip) involved allow for a wide variety of postures that can be assumed in order to maintain CoG
Instance of musculoskeletal abnormality • Damaged tissue result in reduced joint ROM causing a decrease in the LOS & placing individual at a greater risk for fall • Research indicates that sensory proprioceptive function is affected when athletes are injured
Assessment of Balance • Subjective Assessment • Romberg Test – traditional assessment • Balance Error Scoring System (BESS) Prentice, 2004, 4th ed. Google Images
Semi-dynamic & dynamic tests • functional reach tests • timed agility tests • carioca • hop test • Timed T-band kicks • Timed balance beam walks (eyes open & closed)
Objective Assessment • Balance systems • Provide for quantitative assessment & training static & dynamic balance • Easy, practical & cost-effective • Utilize to assess: • Possible abnormalities due to injury • Isolate various systems that are affected • Develop recovery curves based on quantitative measures in order to determine readiness to return • Train injured athlete • Computer interfaced force-plate technology • Vertical position of CoG is calculated • Vertical position of CoG movement = indirect measure of postural sway
Prentice, 2004, 4th ed. • Force plate measures • Allows for static & dynamic postural assessment • Single or double leg stance, eyes opened or closed
Dynamic stability- Ability to transfer vertical projection of CoG around a stationary supporting base • Perception of safe limit of stability • Athlete should maintain their CoP near A-P and M-L midlines
Injury & Balance • Stretched/damaged ligaments fail to provide adequate neural feedback, contributing to decreased balance & proprioception • May result in excessive joint loading • Could interfere with transmission of afferent impulses • Alters afferent neural code conveyed to CNS • Decreased reflex excitation • Caused via a decrease in proprioceptive CNS input • May be the result of increased activation of inhibitory interneurons within the spinal cord • All of these factors may lead to progressive degeneration of joint & continued deficits in joint dynamics, balance & coordination
Ankles • Joint receptors believed to be damaged during injury to lateral ligaments • Knee Injuries • Ligamentous injury has been shown to alter joint position detection • Head Injury
Balance Training • Vital for successful return to competition from lower leg injury • Possibility of compensatory weight shifts and gait changes resulting in balance deficits • Functional rehabilitation should occur in the closed kinetic chain – nature of sport • Adequate AND safe function in the open chain is critical = first step in rehabilitation
Rules of Balance Training • Exercise must be safe & challenging • Stress multiple planes of motion • Incorporate a multisensory approach • Begin with static, bilateral & stable surfaces & progress to dynamic, unilateral & unstable surfaces • Progress towards sports specific exercises • Utilize open areas • Assistive devices should be in arms reach early on • Sets and repetitions • 2-3 sets, 15 → 30 repetitions or • 10 of the exercise for 15 → 30 seconds later on in the program
Classification of Balance Exercises • Static - • CoG is maintained over a fixed base of support, on a stable surface • Semi-dynamic • Person maintains CoG over a fixed base of support while on a moving surface • Person transfers CoG over a fixed base of support to selected ranges and or directions within the LOS, while on a stable surface • Dynamic • Maintenance of CoG within LOS over a moving base of support while on a stable surface • Functional • Same as dynamic with inclusion of sports specific task
Prentice, 2004, 4th ed. • Phase I • Non-ballistic types of drills • Static balance training • Bilateral to unilateral on both involved & uninvolved sides • Utilize multiple surfaces to safely challenge athlete & maintaining motivation • With & without arms/counterbalance • Eyes open & closed • Alterations in various sensory information • Incorporation of multiaxial devices • Train reflex stabilization & postural orientation
Phase II • Transition from static to dynamic • Running, jumping and cutting – activities that require the athlete to repetitively lose and gain balance in order to perform activity • Incorporate when sufficient healing has occurred • Semi-dynamic exercised should be introduced in the transition • Involve displacement or perturbation of CoG • Bilateral, unilateral stances or weight transfers involved • Sit-stand exercises, focus on postural
Bilateral Stance Exercises Prentice, 2004, 4th ed.
Prentice, 2004, 4th ed. • Unilateral Semi-dynamic exercises • Emphasize controlled hip flexion, smooth controlled motion • Single leg squats, step ups (sagittal or transverse plane) • Step-Up-And-Over activities • Introduction to Theraband kicks • Balance Beam • Balance Shoes
Phase III • Dynamic & functional types of exercise • Slow to fast, low to high force, controlled to uncontrolled • Dependent on sport athlete is involved in • Start with bilateral jumping drills – straight plane jumping patterns • Advance to diagonal jumping patterns • Increase length and sequences of patterns • Progress to unilateral drills • Pain & fatigue should not be much of a factor • Can also add a vertical component to the drills • Addition of implements • Tubing, foam roll • Final step = functional activity with subconscious dynamic control/balance
Phase III Exercises Prentice, 2004, 4th ed.
The dynamic proprioceptive re-education consists of seven stages:- • Slow exercises followed by quicker movement • Exercise with limited effort followed by exercises requiring greater strength • Exercises requiring volition, followed by exercises done freely • Progress from walking to jogging • Running and sprinting • Jumping and changes of direction • Twirling and twisting around the injured or operated knee
Balance and control proprioceptive exercises • Stand on one leg. • Stand on one leg with eyes closed. • Stand on one leg – throw and catch a ball. • Stand on one leg – bend and straighten knee
Stand on one leg- pick up item from floor. • Hold knee dip – throw and catch a ball. • Stand on one leg – move other leg to side, front and back. • Push up onto toes (2 legs) and hold. • Push up onto toes with eyes closed. • Push back onto heels, balance and hold. • Push up on toes on one leg.
Walking proprioceptive exercises • Walk forward along a straight line. • Walk on tip toes along straight line. • Walk backwards along straight line. • Side step along straight line. • Walk sideways crossing one foot over other (Cariocas). • Walk fast in one direction, quickly changing direction at intervals.
Running proprioceptive exercises • Run fast in one direction. • Run backwards and do sidesteps. • Fast crossovers (Cariocas). • Run in figure of eight – make it smaller and smaller.
Hopping on spot • Hop forwards and backwards – stop between hops. • Hop in zigzags. • Hop on and off step • Do triple jump - run, hop, jump and land.
Balance and strength exercises are combined by incorporating light external forces and increasing the level of difficulty for balancing while strengthening the muscles required for dynamic stabilization
Plyometrics begin with low-impact hopping, progressing to double-leg bounding, and finally single-leg hopping.
References • Prentice, W.E. (2004). Rehabilitation Techniques for Sports Medicine and Athletic Training, 4th ed., McGraw-Hill • Houglum, P.A. (2005). Therapeutic Exercise for Musculoskeletal Injuries, 2nd ed., Human Kinetics. • Kisner, C. & Colby, L. (2002). Therapeutic Exercise Foundations & Techniques, 4th ed., F.A. Davis. • http://www.google.com - Images