Gram-Negative Rods
Gram-Negative Rods. General Classification. Based on source or site of infection 1. Enteric tract 2. Respiratory tract 3. Animal sources. Source or site of infection. Enteric tract Both within and outside: Escherichia, Salmonella Primarily within: Shigella , vibrio , Campylobacter

Gram-Negative Rods
E N D
Presentation Transcript
General Classification • Based on source or site of infection 1. Enteric tract 2. Respiratory tract 3. Animal sources
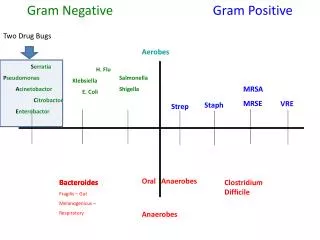
Source or site of infection • Enteric tract Both within and outside: Escherichia, Salmonella Primarily within: Shigella, vibrio, Campylobacter Outside only: Klebsiella-Enterobacter-Serratia group, Proteus-Providencia-Morganella group, Pseudomonas, Bacteroides
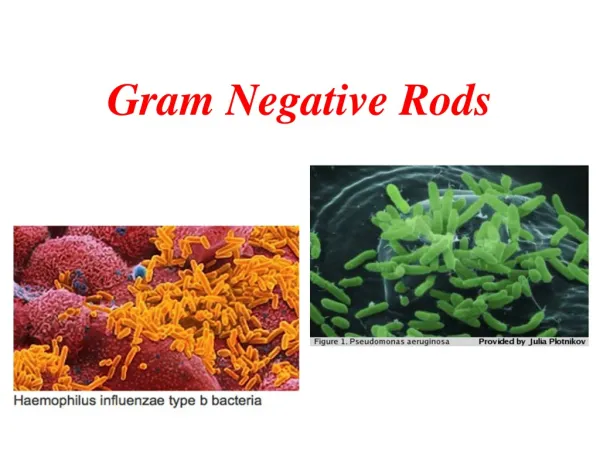
Source or site of infection (continued) • Respiratory tract: Haemophilus, Legionella, Bordetella • Animal sources: Brucella, Francisella, Pasteurella, Yersinia
Classification Based on morphology, biochemical traits and genetic (phylogenetic) relationship • Enterobacteriaceae • Pseudomonaseae • Vibrionaceae • Cocobacilli
Enterobacteriaceae • A heterogenous family • Mostly found in colon of human and other animals • Different pathogenetic mechanisms • Facultative anaerobic • Glucose fermentation • None have cytochromeoxidase • Reduce nitrates to nitrites
Most important genusesin Enterobacteriaceae family • Escherichia • Shigella • Salmonella • Klebsiella • Enterobacter • Serratia • Proteus • Yersinia
In contrast to Enterobacteriaceae • Pseudomonas Gram negative rods: • Non-fermenting (Strict aerobic) • Not reduce nitrate • Oxidase-positive
General structure of cells in Enterobacteriaceae • All have Endotoxin • Some have Exotoxins, mostly called enterotoxins • Three surface antigens: O antigen: outer polysaccharide portion of the lipopolysaccharide (repeating 3-4 oligosaccharide sugars 15-20 times). A basis for the serologic typing (about 2000 types of Salmonella and 150 types of E. coli). H antigen:on the flagellar protein (in E.coliand Salmonella and not in Klebsiella and shigella). Unusual H antigens in Salmonella called phase 1 and phase 2. The organism can reversibly change in antigenicity to evade the immune response. K polysaccharide antigen: In encapsulated organisms such as Klebsiella. Identified by quellung(capsular swelling) reaction in the presence of specific antiseraused for epidemiologic purposes. In S. typhi, it is called Vi (or virulence) antigen.
Laboratory diagnosis • Culture for isolation Suspected specimens are inoculated onto 2 media: 1. Blood Agar 2. A selective differential medium (MacConkey’s agar or eosin-methylene blue, EMB agar. The differential ability is based on lactose fermentation as the most important criterion in identification of these organism. Non lactose fermenters form colorless colonies. Selective effect is exerted by bile salts or bacteriostatic dyes
Laboratory diagnosis (continued) • Culture for identification • Screening biochemical tests for a final definitive identification: Triple sugar Iron Agar (TSI) Almost enough to identify the genus but array of 20 or more biochemical tests to identify the species.
Triple Sugar Iron Agar and Urea Agar Triple Sugar Iron Agar • Indicator : Phenol red. • Components: - Iron or Ferrous sulfate - 3 sugars: glucose, lactose, and sucrose • Black FeS indicates the production of SH2 (Ferrous sulfate + Solfate reductase ferro sulphide (Sfe)
Urea AgarIndicator: Phenol red. Component : Urea If the bacterium Produces urease: Urea is hydrolyzed to NH3and CO2 ---> light orange changes to reddish purple (in Proteus and K pneumoniae
Amonium citrate (Simmons Citrate) Indicator: Bromothymol blue If the bacterium can utilizes ammonium dihydrogen phosphate (a salt of ammonium) and sodium citrate as sole source of nitrogen and carbon, the indicator turns to blue at alkalin pH due to releasing ammonia.
Motility • SIM medium: SH2, Indole, Motility • Proteus: Swarms • Differentiation between Enterobacter cloacae (motile) from Klebsiellapneumoniae (Non motile)
Indole • Tryptophan Tryptophanase Deamination Intermediate products: Indole + …. • Detection: 5 drops Kovac’s reagent (contains paradimethlaminobenzaldehyde = PDAB) is added Red ring
Serology Usually in Salmonella, Shigella and E.colifinal detection (serotyping) by agglutination Ag+Ab test.
Coliforms • That part of this family which are normal inhabitants of the colon: E. coli Enterobacter Klebsiella Citrobacter So, E.coli is the indicator for fecal contamination of water supply: Lactose fermentation, Acid and gas production, growth at 44.5 C and typical colony on EMB. 4 colony count per dL in drinking water is indicative of unacceptable fecal contamination.
Antibiotic therapy • Must be individually tailored to the antibiotic sensitivity test (Antibiogram). • Penicillin and cephalosporin families. Aminoglycosides (Gentamicin, amikacin, kanamycin, streptomycin …), Chloramphenicol, tetracyclines, quinolones and sulfonamides.
Escherichia coli • Diseases • Diarrhea or dysentery • UTI 2. The most common cause of sepsis among negative rods 3. One of the 2 important causes of neonatal meningititis (the other is the group B streptococci) due to colonization of vagina by these organisms in about 25% of pregnant women.
Virolence factors: • Pili • Capsule • Endotoxin • Two exotoxins (enterotoxins).
E. colipili (fimbriae) mannose • galactose • glycolipids • glycoproteins
Pathogenesis • E. coli attaches to the surface of jejunum and ileum by Pili Bacteria synthesize enterotoxins (exotoxins determined by plasmids) Diarrhea • The toxins are strikingly cell-specific: Cells of colon are not susceptible due to lack of receptors for the toxins.
EnteropathogenicE. coli (EPEC) • EnterotoxigenicE. coli (ETEC) • EnteroinvasiveE. coli (EIEC) • EnterohemorrhagicE. coli (EHEC)
EnteropathogenicE. coli (EPEC) • destruction of surface microvilli • fever • diarrhea • vomiting • nausea • non-bloody stools • Diarrhea is self-limited and short duration (1-3 days) Gut lumen
EnterotoxigenicE. coli • Travellers diarrhea • Diarrhea like cholera but milder • Diarrhea is self-limited and short duration (1-3 days)
EnterotoxigenicE. coli (ETEC) • Heat labile toxin (LT) • like choleragen • Adenylatecyclase activated • cyclic AMP concentration • secretion water/ions (potassium and chloride) • Heat stable toxin (ST) • Guanylatecyclase activated • cyclic GMP concentration • uptake water/ions (Sodium and Chloride)
EnterohemorrhagicE. coli (EHEC) • Produce verotoxin which works like Shiga toxin • Hemorrhagic • bloody, copious diarrhea • few leukocytes • hemolytic-uremic syndrome • hemolytic anemia • thrombocytopenia (low platelets) • kidney failure
Transmission electron micrograph Enterohemorrhagic E. coli • Usually O157:H7 Flagella
EnteroinvasiveE. coli (EIEC) Very similar to Shigella species (in biochemical and morphological traits) • Non lactose fermantative • Non motile • Invades to epithelial mucosal cells • Cause enteric inflammation
E. coli Transmission Meat products or sewage-contaminated vegetables
UTI • The most common agent for UTI (Cystitis, pyelonephritis): fever, chills, flank pain • Occurs primarily in women Attributed to 3 features which facilitate ascending infection into bladder: • A short urethra • Proximity of the urethra to the anus • Colonization of vagina by members of fecal flora. • The most frequent cause of nosocomial UTI. (equally in both men and women and associated with using catheters)
Systemic infection • Capsule and endotoxin play a prominent role • Capsular polysaccharide interferes with phagocytosis (Serotype having K1 causes neonatal meningitis). • LPS during sepsis causes fever, hypotension and disseminated intravascular coagulation.
Treatment • Antibiogram for most infections • A combination of ampicillin and gentamicin in neonatal meningitis • Rehydration for diarrhea
Prevention • No passive or active immunisation • Prompt withdraw of catheters and intravenous lines • Caution regarding uncooked food and unpurified water while traveling.
Shigella • Important properties • Non lactose fermenting • Distiguishable from Salmonella by: no gas, no H2S, nonmotile. • Divided into 4 groups based on O antigen: A, B, C and D. • Having an enterotoxin called Shiga toxin
Disease: Shigellosis • Only a human disease • Transmitted from person to person by asymptomatic carriers (oral fecal transmission) • 4 F’s – fingers, flies, food, feces • Food-born outbreaks outnumber water-born outbreaks by 2 to 1. • In mental hospitals and day-care nurseries • Children <7 accounts for half of shigella positive stool culture
Pathogenesis • Exclusively in gastrointestinal tract • Bloody diarrhea (dysentery): Invading the mucosa of the distal ileum and colon. • Local inflammation accompanied by ulceration occurs, but the organisms rarely penetrate the wall or enter the bloodstream unlike salmonellae. • Although some have an enterotoxin, invasion is not only due to enterotoxin.
Most invasive species • S. dysenteriae causes the most severe disease but S. sonnei causes mild disease but more frequent
Clinical findings • Incubation period: 1-4 days • Symptoms: Fever, abdominal cramps, followed by diarrhea (watery at first but later contains blood and mucus). • It can be mild or severe depending 2 major factor: The species of Shigella and the age of the patient.
Clinical findings • Resolves in 2-3 days but antibiotic can shorten the course. • Serum agglutinins appear after recovery but are not protective because the organism does not enter the blood.
Lab diagnosis • Non-lactose fermenting…… • Slide agglutination to detect its group • Methylene blue stain of a fecal sample to determine whether PMNs are present: An invasive one: Shigella, Salmonella or Campylobacter rather than a toxin-producing organism such as V. cholerae, E. coli or Clostridium perfringens or certain viruses or Entamoeba histolytica.
Treatment • The main treatment: Fluid and electrolyte replacement. • No antibiotic in mild cases • Antibiogram test: Trimethoprim - sulfamethoxazole or ampiciln. • Antiperistaltic drugs are contraindicated as they prolong the fever, diarrhea an excretion.
Prevention • Interruption of fecal-oral transmission by proper sewage disposal, chlorination of water and personal hygiene. • No vaccine • Antibiotic prophylactic is not recommended.
Salmonella Important properties • Not ferment lactose • Produce H2S, Gas, motile
Naming the salmonella • S. typhi • S. paratyphi (A, B, C…) • S. typhimurium • S. choleraesuis • S. enteritidis (1500 serotypes)
Diseases - Enterocolitis (S. typhimurium) - Enteric fever (typhoid fever) (S. typhi and S. paratyphi) - Septicemia with metastatic abscesses (S. choleraesuis)