Download

1 / 127
1.28k likes | 1.72k Vues
Surgical Pathology Unknown Conference. Kelley E. Capocelli, MD October 15, 2007. CASE #1. Case #1. Seventeen year old male with six month history of left chest pain, most noticeable when taking a deep breath

E N D
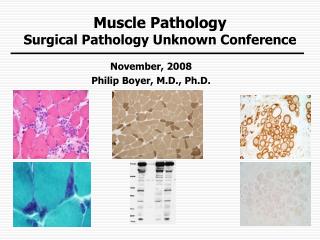
Surgical Pathology Unknown Conference Kelley E. Capocelli, MD October 15, 2007
Case #1 • Seventeen year old male with six month history of left chest pain, most noticeable when taking a deep breath • Chest x-ray showed a lytic lesion with sclerotic margins arising from the posterior aspect of the left 7th rib • Expansion of bone with thinned but intact cortex
Diagnosis • Periosteal chondroma • A benign cartilaginous lesion characterized by its location on the metaphyseal cortex of both the long and short tubular bones • Develops in the periosteal region, frequently eroding the cortex
Periosteal chondroma • Although these tumors can occur both in adults and children, they predominate in patients younger than 30 years, with the highest frequency in the second decade • The most common location for periosteal chondromas are in the metaphyses of long tubular bones, particularly the proximal humerus, although small tubular bones of hands and feet can also be involved
Periosteal chondroma • Nojima et al reported only 46 periosteal chondromas among a total of 7,000 cases of primary bone tumors on file at the Mayo clinic and only 2 of these originated in the rib • Most chondromas are centrally located in the bone and are called enchondromas • About 20% are eccentric and arise on the cortex underneath the periosteum and are called periosteal chondromas
Case #2 • Ten year old female with a history of JRA presents with left sided chest pain X 2-3 weeks. • Pain started out as a dull ache but became more sharp and pleuritic in nature, especially during coughing, deep inspiration, sneezing, and leaning forward. • Chest x-ray showed a large soft tissue mass that appeared to be arising from the left 4th rib
Diagnosis • Conventional osteosarcoma, chondroblastic type • Cartilaginous matrix production is evident throughout most of the tumor. • While the majority of the tumor tends to be of lower grade, some of the chondroid areas contain cytologically atypical cells that are characteristic of higher-grade tumors. • These chondroblastic foci are admixed with malignant spindle cells that produce osteoid trabecula. • Malignant osteoid with a filigree pattern is seen focally
Conventional Osteosarcoma • The most common primary malignancy of bone in children and adolescents • The fifth most common malignancy among adolescents and young adults aged 15 to 19 • Accounts for only 5 percent of childhood cancers overall
Conventional Osteosarcoma • Depending upon the predominant cellular component, conventional osteosarcomas are subclassified as: • Osteoblastic (accounting for 50 percent of conventional osteosarcomas) • Chondroblastic (25 percent) • Fibroblastic (25 percent)
Conventional Osteosarcoma • Bimodal age distribution of osteosarcoma incidence • Early adolescence (the peak incidence is between 13 and 16 years of age) • Appears to coincide with the adolescent growth spurt • More common in boys than girls • Adults over the age of 65
Conventional Osteosarcoma • The tumor appears most frequently at sites where the greatest increase in bone length and size occurs (the metaphyseal portions of the distal femur, proximal tibia, and proximal humerus) • Osteosarcomas occur at an earlier age in girls, corresponding to their more advanced skeletal age and earlier adolescent growth spurt.
Conventional Osteosarcoma • Typical radiograph appearance: • Destruction of the normal trabecular bone pattern • Indistinct margins • No endosteal bone response. • The affected bone is characterized by a mixture of radiodense and radiolucent areas, with periosteal new bone formation, lifting of the cortex, and formation of Codman's triangle
Conventional Osteosarcoma • Tumors are typically removed after 5-6 cycles of chemotherapy • Percentage of tumor viability post treatment is used to predict outcome • Depending on the location and age of the patient, radiation therapy may also be utilized
Back to our patient • Approximately 50% of this patient’s tumor remained viable after chemotherapy, indicating poor response to treatment
Case #3 • Eight year old boy with complaint of right thigh pain x 6 months • Right thigh larger circumference than left thigh • Initially presented with right calf atrophy • At time of second biopsy was noted to have right calf fullness • Neurologic deficits
Are there any immunohistochemical stains that might help with the diagnosis?
Diagnosis • Malignant peripheral nerve sheath tumor • Involving the sciatic nerve, common peroneal nerve, tibial nerve, and lateral plantar nerve • Surgical margins negative for involvement
Malignant peripheral nerve sheath tumor • Sarcoma arising within the peripheral nervous system • As defined by the WHO, MPNST refers to any malignant tumor that arises from the nerve sheath or shows features of nerve sheath differentiation • Tumor cells do not often show immunohistochemical characteristics of Schwann cells such as S100-protein expression
Malignant peripheral nerve sheath tumor • Often occur in the presence of Neurofibromatosis type 1 • Commonly arising in plexiform neurofibromas • The lifetime risk of MPNST developing in NF1 patients has been estimated at 8% to 13%, as compared with 0.001% in the general population • Histologic clue – tumor cells are vasculocentric (vessel loving)