Download

1 / 77
800 likes | 1.24k Vues
ANTERIOR MEDIASTINUM Surgical pathology. The 3 rd . Surgical Unit Feb.2009. Limits of the superior mediastinum. anterior - manubrium of the sternum posterior - anterior surface of bodies of vertebrae T1-T4 superior - plane of the thoracic inlet

E N D
ANTERIOR MEDIASTINUMSurgical pathology The 3rd. Surgical Unit Feb.2009
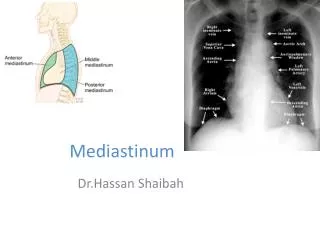
Limits of the superior mediastinum anterior - manubrium of the sternum posterior - anterior surface of bodies of vertebrae T1-T4 superior - plane of the thoracic inlet inferior - plane of the sternal angle lateral - mediastinal pleura
Planes in the superior mediastinum from anterior to posterior • glandular plane • venous plane • arterial-nervous plane • visceral plane • lymphatic plane
Manubrium of the sternum + the cartilage of the first rib = anterior boundary of the A-S mediastinum
The first plane is the glandular plane. It consists of two lobes and is mainly fat in the adult with small islets of active thymic cells scattered throughout
The second plane is the venous plane and consists of the: left brachiocephalic vein, right brachiocephalic vein, SVC
The third plane is the arterial-nervous plane aortic arch and its branches : brachiocephalic artery, left common carotid artery, left subclavian artery nerves: left and right vagus nerves, left and right phrenic nerves
The fourth plane is the visceral plane trachea , esophagus , left recurrent laryngeal nerve
COMPARTIMENT ANTERO-SUPERIOR • Fascia endotoracica • Timus • Trunchiuri venoase brahio-cefalice- VCS • Crosa aortei • Ganglioni mediastinali sup. • Nervii vagi • Nervii recurenti • Nervii frenici
LOJA TIMICA-rapoarte • Anterior: • Art. sterno-condro-claviculara • Manubriul sternal • M. subhioidieni • Fata post. lig. sterno-pericardic sup. • Posterior: • Lama tiro-aorto-pericardica: • Tr. v. br.-cef., VCS, tr. a.br.-cef., carotida stg. • Pericard
TIMUS Marginit de sinusurile pleurale anterioare Inconjurat de o capsula fibroasa Periglandular- tesut conj. lax- disectie usoara Aderentele –lig. timo-tiroidian si timo-pericardic
TIMUS-rapoarte • Regiunea cervicala • Anterior: m. subhiodieni • Posterior: trahee, vene tir. inf. • Lateral: a. carotida comuna, vena jugulara interna, nervul vag
TIMUS-rapoarte • Mediastinul anterior • Anterior: sternul+ primele 4-5 cartilaje costale, vase toracice interne • Posterior: pericard, n.cardiaci, tr. pulmonar, aorta ascendenta, crosa, ramuri, VCS, v. br.-cef. • Lateral: pleure M., nervi frenici, vase frenice sup.
TIMUS-vascularizatie • Pedicul superior: art. timice sup. din art. tiroidiana inf. • Pedicul lateral: art.timice lat. din art. toracice interne sau dfg. sup. • Pedicul mijlociu: art. timica mijlocie din trunchi art. brahiocefalic sau aorta
TIMUS-vascularizatie, inervatie • Venele timice- tr. venos br-cef., 2mm diam, scurte- punct critic • Limfaticele- ggl.parasternali, jugulari, bronho-mediastinali- duct toracic • Nervii timici- din vag, lant simpatic cervico-toracic si frenic
GUIDELINES Whenever you see a mass on a chest x-ray that is possibly located within the mediastinum, your goal is to determine the following: • Is it a mediastinal mass? • Is it in the anterior, middle or posterior mediastinum? • Are you able to characterize the lesion by determining whether it has any fatty, fluid or vascular components?
Statistically, it is important to remember the following: Most masses (> 60%) are: • Thymomas • NeurogenicTumors • Benign Cysts • Lymphadenopathy (LAD) • In children the most common (> 80%) are: • Neurogenictumors • Germ cell tumors • In adults the most common are: • Lymphomas • LAD • Thymomas • Thyroid masses
Localize to the mediastinum Left. A lung mass abutts the mediastinal surface and creates acute angles with the lung. Right. A mediastinal mass will sit under the surface of the mediastinum, creating obtuse angles with the lung.
Localize within the mediastinum • The mediastinum can be divided into anterior, middle and posterior compartments.It is important to remember that there is no tissue plane separating these compartments. • On the lateral radiograph the anterior and middle compartments can be separated by drawing an imaginary line anterior to the trachea and posteriorly to the inferior vena cava. • The middle and posterior compartments can be separated by an imaginary line passing 1 cm posteriorly to the anterior border of the vertebral bodies.This division allows us to make a more narrow differential diagnosis.
On the PA film there is a lobulated widening of the superior mediastinum.On the lateral chest film the retrosternal clear space is obliterated.This happened to be a patient with lymphoma.
FDG-PET images of the same patient.There are multiple lymphatic masses in the anterior, middle and even posterior mediastinum, spreading to the neck.
On the chest film there is a mass that has obtuse angles with the mediastinum, so it is a mediastinal mass.The anterior location was confirmed on a CT.Most commonly this will be a mass of thymic or lymphatic origin.This proved to be a lymphoma in a HIV-positive patient.
Substernal parathyroid adenoma CT revealed an encapsulated mass of 3 cm in the upper anterior mediastinum behind the sternum-clavicular joints, with marked peripheral enhancement (arrow).
Tc-99m-sestamibi substraction image showed an area of intense uptake below the inferior pole of the left thyroid lobe, in the upper mediastinum, in the left median position and normal thyroid with homogenous radiopharmaceutical uptake (arrow)
Cystic masses The anterior mediastinum is an important location for cystic masses. Masses can be entirely cystic (thymic cysts) or have solid components (lymphoma or cystic thymoma). Some masses are cystic with enhancing septations - in these cases you should think of a germ cell tumor.
The CT shows an anterior mediastinal mass with water density attenuation.This is typical for a thymic cyst.
The CT shows a mass located in the anterior mediastinum.The mass is cystic but has solid enhancing septa.This finding is very specific for a germ cell tumor.
The CT shows a mass located in the anterior mediastinum.The mass is cystic but has solid enhancing components, so ? lymphoma, germ cell tumor and cystic thymoma.This proved to be a cystic thymoma.
LEZIUNI TIMICE TIMUS HIPERPLAZIC TIMUS ATROFIC TUMORI TIMICE TIMUS NORMAL +/- MIASTENIA GRAVIS sau alte BOLI AUTOIMUNE
MIASTENIA GRAVISDefinitie, Kirschner, 1991 • Clinic- fatigabilitatea muschilor voluntari la efort repetitiv, cu refacere la odihna • Electrofiziologic- raspuns decrement la stimularea repetitiva-EMG • Farmacologic- raspuns pozitiv la tensilon • Patologic- modificari histo-pat. timice si structurale la nivelul R. Ach. si placa n-m. • Imunologic- prezenta Ac. antiR Ach. si raspuns favorabil la imunosupresie
NA, 39ani, MG-Oss-IV (6 ani istoric)op.12-III-1997, AP-HLT, deces- 20.III.1997
MIASTENIA GRAVIS • Boala autoimuna dobindita – necunoscute??? • Ce declanseaza aparitia bolii? • De ce sunt miastenici sero-negativi? • De ce exista variabilitate mare de raspuns la tratament: remisie completa, remisie farmacologica, ameliorare, agravare, fara raspuns, deces- insuf. resp. acuta? • De ce un timus normal poate induce boala? • De ce apare miastenia dupa indepartarea unui timom?
MIASTENIA GRAVIS • Tratamentul- nu este inca standardizat; • Discipline implicate in management: neurologie, imunopatologie, histopatologie, endocrinologie, radiologie, medicina nucleara, chirurgie, anesteziologie, oncologie ( radioterapeut, chimioterapeut)
CAI DE ABORDMEDIASTINUL ANTERIOR • TORACOTOMIE • STERNOTOMIE • CERVICOTOMIE • ABORD MIXT • TORACOSCOPIC • MEDIASTINOSCOPIC
TORACOTOMIA ANTERO-LATERALA • AVANTAJE: • Poate fi prelungita posterior • Poate fi prelungita prin sectiunea transversala a sternului • Poate fi asociata cu o cervicotomie • Expune bine pediculul pulmonar si vasele mari • Incizie estetica situata in santul submamar • DEZAVANTAJE • Acces dificil pentru planul traheo-bronsic • extremitatea sa interna ramine un punct slab, greu de inchis