Download
1 / 40
420 likes | 479 Vues
This case study presents a 23-year-old male involved in a high-speed car crash with concerns of genitourinary trauma. Learn about assessment, concerns, useful diagnostic tools, and management approaches for urethral and bladder injuries, hematuria, and kidney trauma.

E N D
Case • 23 y.o male • Driver, Seatbelted • Frontal Impact, High Speed ( 100Km/h) • Airbag + • Other driver dead • Car completely destroyed • Patient was conscious at the scene. • On scene: BP=85/50 HR:120 RR:22 Sat:98%
cont. • A: Clear. C-spine protection. Backboard+ • B: A/E symetric. O2 Sat N. No crepitus. Trachea central. • C: BP:100/60 HR:100 Mentating well. • D: GCS=15 • Pt is exposed. • O2 - iv – monitor • Temperature N Capillary Glucose N
cont. • AMPLE • C/O abdo. Pain + “hip” pain • C/O right lower leg pain • Secondary Survey • Spleen normal. Mild suprapubic tenderness. • Pelvic instability • Probable right tibial # • No gross blood at meatus. Rectal Normal. • “Doctor, can I put a Foley?”
cont. • What are your concerns? • Foley? • What will be the usefulness of dipstick? • Dipstick good enough? U/A? • What if he has microscopic hematuria? • What if he has a pelvic fracture? • Any different if you had blood at meatus? • Urethrogram? Cystogram? Abdominal CT? • Worried about the kidneys? Bladder? • Does the low BP changes your suspicion for a GU injury?
Introduction • GU Trauma overlooked • 10-20% of all injured patients • Long term morbidity • Impotence • Incontinence • Life-threatening injuries first
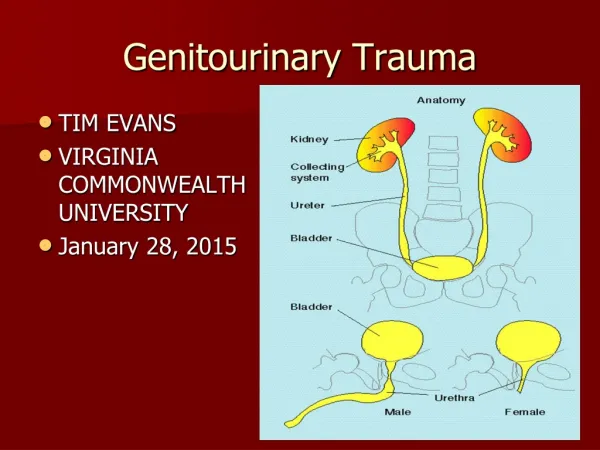
Plan • Urethral Injury • Bladder Injury • Hematuria in Trauma • Kidney Injury
Definitions • Upper tract • Kydney • Ureters • Lower tract • Bladder • Urethra • External genitalia
Urethral Trauma • Almost exclusively in male • Significant morbidity • Stricture • Incontinence • Impotence • If unrecognized: • Converting partial to complete tear • Inaccurate assessment of U/O • Foley catheter implication Andrich DE et al. The nature of urethral injury in cases of pelvic fracture urethral trauma. Journal of Urology. 165(5):1492-5, 2001 May.
Anatomy Bladder Symphysis
Prostatic Membranous Bulbous Pendulous
Clinical Features • Gross hematuria in 98% • Inability to void • Blood at urethral meatus • Pelvic / suprapubic tenderness • Penile / scrotal / perineal hematoma • Boggy / high-riding prostate/ ill-defined mass on rectal examination.
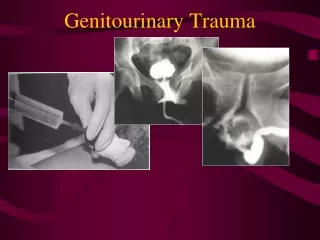
Posterior Urethral rupture From McAnich JW. In Tanagho EA, McAninch JW, editors: Smith’s general urology, ed 14, Norwalk, Conn, 1995, Appleton & Lange.
Diagnosis:Retrograde Urethrogram • Pretest KUB film • Supine position • Injection of 60ml of water-soluble contrast • Different techniques • X-ray when 10ml left and after 60ml • Post-voiding x-ray.
Retrograde Urethrogram:Interpretation • Contrast extravasation + Contrast in bladder • Contrast extravasation only PARTIAL Tear COMPLETE Tear
Management • Partial tear • careful passage of 12-14 Fr. Foley. • If any resistance: Urology • Complete tear: • Urology + suprapubic cath. • If Foley already there and suspect tear: • LEAVE FOLEY IN PLACE • Small feeding tube alongside the foley
Foley Catheter • NO if you suspect a urethral injury • Most of urethral injuries: Pelvic # or Gross hematuria • Initial bladder effluent MUST be looked at. • Danger to convert partial into complete • Successful passage complete tear • NEVER REMOVE A FOLEY WHEN YOU SUSPECT A PARTIAL TEAR AFTERWARDS. • ANY colored urine other that yellow = BLOOD until proven otherwise
Bladder Trauma • Adult: Extraperitoneal organ • Bladder dome = weakest point • Blunt: 60-85% • MVA: #1 cause • Important to recognize • Pelvic/abdominal wall abscess/necrosis • Peritonitis • Intra-abdominal abscess • Sepsis / Death
Types of rupture • Extraperitoneal • Most common • Pelvic # in 89-100% • Bladder rupture in 5-10% of all pelvic # • Intraperitoneal • Extravasation of urine in abdomen • Sudden force to full bladder • Associated injuries +++ Mortality (20%)
Investigation • Cystography: Gold standard • CT Cystography : New trend
Treatment • Penetrating injuries: OR • Blunt • Intraperitoneal: Almost all OR • Extraperitoneal: Urethral cath. drainage
Kidney Injury • Retroperitoneal organ • Cushoned by perinephric fat • Gerota’s fascia • Along T10 - L4 • Ribs 10-12 • Fixed only through pedicle. • 1.2L of blood / min
Kidney Injury… • Blunt trauma: 80-90% • Rapid deceleration / Direct blow • MUST be suspected if • Trauma to back / flank / lower thorax / upper abdomen • Flank pain / low rib # • Hematuria / Ecchymosis over the flanks • Sudden decelaration / Fall from height. • Lumbar transverse process #
Grade I • Contusion • Hematuria • Urologic studies N • Hematoma • Subcapsular • Non expanding • Parenchyma N
Grade II • Hematoma • Perirenal • Nonexpanding • Laceration • < 1.0 cm • Renal cortex only • No urinary extravasation
Grade III • Laceration • > 1.0 cm • Renal cortex only • No urinary extravasation • Intact collecting system
Grade IV • Laceration • Renal cortex • Renal medulla • Collecting system • Vascular • Main renal artery/vein injury with contained hemorrage.
Grade V • Completely shattered kidney. • Avulsion of renal hilum (pedicule) which devascularizes kidney. Kennon et al. Radiographic assessment of renal trauma: our 15-year experience. The Journal of Trauma, 154: 353-355; August 1995.
Investigation • IVP • Used to be intial exam of choice. • Very poor sensitivity for penetrating injury • Limitation in staging renal injuries • Not 1st choice anymore. Only if pt unstable. • Contrast CT • Study of choice if stable • More sensitive and specific for staging • Detects other abdominal injuries
Management • Penetrating trauma: • Imaging for ALL (9%: NO hematuria) • Blunt trauma Imaging: • Gross hematuria • Microscopic hematuria (5 RBC/hpf) + shock (BPs90) • Any child with > 50 RBC / hpf • Acceleration decceleration • Pelvic FX
Management… • Absolute indication for Surgery: • Uncontrollable renal hemorrage • Multiply lacerated, shattered kidney • Main renal vessels avulsed • Penetrating injuries usually • Grade I-II • conservative • Grade III-IV • Conservative if stable hemodynamically vs. surgery • Grade V • Surgery Grade V
Back to case • First urine: Dipstick +++ (15 RBC/hpf) • Pelvic x-ray: Straddle #
Kozin, Berlet. Handbook of Common Orthopaedic Fractures, 4th ed., 2000.
case • First urine: Dipstick +++ (15 RBC/hpf) • Pelvic x-ray: Straddle # • Keypoints… • BP: 85/50 on scene • Microhematuria • Pelvic # • NO FOLEY
case • Urology consulted • Retrograde urethrogram: N • CT cystogram: N • Contrast CT to look for renal injury: Grade II renal injury.
Conclusion • No Foley if you suspect urethral trauma • Gross hematuria OR microhematuria + Shock = GU Trauma. • Pelvic # + Microhematuria GU investigation • Don’t remove Foley if you suspect a partial tear of urethra afterwards. • Microhematuria alone : No imaging …but F/U. • In peds: Imaging for ALL hematuria.
The End The End