GENITOURINARY TRAUMA
GENITOURINARY TRAUMA. Mark Boyko EM. Objectives. Key aspects of GU trauma in an anatomical approach: External Genitalia Urethral Injury Bladder Injury Ureteral Injury Renal Injury. GU Trauma. 80% of GU trauma is BLUNT trauma


GENITOURINARY TRAUMA
E N D
Presentation Transcript
GENITOURINARY TRAUMA Mark Boyko EM
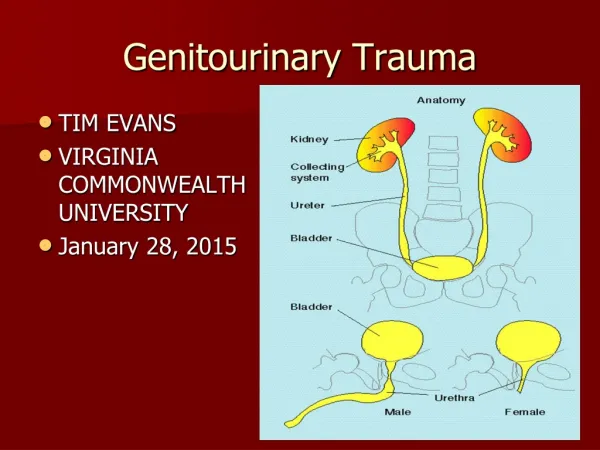
Objectives Key aspects of GU trauma in an anatomical approach: External Genitalia Urethral Injury Bladder Injury Ureteral Injury Renal Injury
GU Trauma • 80% of GU trauma is BLUNT trauma • Very rarely is life threatening, so take a step back and move through your systems anatomically • Assessing for concomitant pelvic fracture is one of the most important points
Eur J Emerg Med. 2004 Aug;11(4):223-4.A human bite to the scrotum: a case report and review of the literature.Kerins M, Greene S, O'Connor N.Emergency Department, St Thomas' Hospital, Lambeth Palace Road, London, SE1 7EH, UK. mkerins_fahey@hotmail.comHuman bites to the scrotum are rare and can be associated with a high morbidity rate if poorly managed. We report a case of a human bite to the scrotum that was successfully treated with a 5-day course of antibiotics, surgical debridement and healing by secondary intention. Anything can happen…
External Genitalia • Trauma here is rare in females • In males, injury is often obvious • Look for swelling, ecchymoses, deformity • Testicular torsion can occur with trauma • Testicular rupture occurs in 50% of patients with a direct blow to a testicle, have a low threshold to ultrasound
Male External Genitalia • Penile Fracture • Usually a ‘sexual accident’ • Immediate pain, often hear a ‘popping sound’, early swelling • Is a rupture of the tunica albuginea surrounding the corpora cavernosa • 20% association with urethral injury • Requires operative repair
Question • A penile fracture is classically described using what vegetable?
Penile Fracture • ‘Eggplant Deformity’
Urethral Injuries • Again, rare in females • In males, divided into ‘anterior’ and ‘posterior’ urethra, divided by urogenital diaphragm
Urethral Injury • In males, 25% of all pelvic fractures have urethral injury (vs only 5% in females), more commonly the posterior division • Gross hematuria and pelvic fracture = posterior urethral injury until proven otherwise • The big 4 clues to urethral injury: • Blood at meatus • Gross hematuria • Inability to void • Ecchymoses, swelling of penis
Question • What 4 things are necessary before you can attempt to pass a foley catheter?
The Great Foley Debate Textbook answer: 4 things allowing you to pass a foley safely: 1. No pelvic and suprapubic tenderness / # 2. No penile, scrotal, or perineal hematoma 3. No blood at the urethral meatus 4. No abnormal findings on DRE
The Great DRE Debate • Textbook answer: • ‘high riding prostate’ or boggy prostate is concerning for a posterior urethral injury • blood causes the prostate to lift superiorly
Is any of this true?? EM Rap 2008 • The Great Foley Debate: • Initial concept came from 1977 paper by a British urologist entitled “A Personal View of Immediate Management of Pelvic Fracture and Ureteral Injury” - no references • UCLA retrospective review of 7 years trauma patients, 46 urethral injuries, 50% of blind passes were successful • The ‘classic’ signs of urethral injury were extremely non-sensitive • One small retrospective review of 13 cases of urethral injury demonstrated no evidence that a blind attempt to insert a urinary catheter worsened the initial injury. • No case reports that passing a foley caused/worsened urethral injury • The Great DRE Debate: -same UCLA retrospective review, 0 had ‘high riding prostates’ -UCLA 1400 trauma patients, more false + DRE’s than true + (for tone, for sensation, for blood)
Urethral Injury - Imaging • If any concern for a urethral injury, do a retrograde urethrogram • Will either be: • Normal • ‘Partial’ urethral injury (some dye in bladder, some extravascation) • ‘Complete’ urethral injury (no dye in bladder)
Urethral Injury - Management • If no concern for injury, or retrograde urethrogram normal, put a foley in. • If a partial urethral tear, textbooks say one careful attempt to pass a 12- or 14-Fr Foley can be undertaken. Most urologists disagree with this, and wish to be consulted. • If a complete tear – suprapubic catheter, urology consult for operative repair.
Bladder Injury Question: Which part of the bladder is the weakest and most likely to rupture? A) Trigone B) Lateral walls C) Dome (superior wall) D) Posterior wall
Bladder Injury • 80% of bladder injuries associated with pelvic # • Injuries classified as: • Contusions • Intra-peritoneal ruptures (through the dome) • Extra-peritoneal ruptures (seen exclusively with pelvic fractures)
Bladder Injury • Signs • GROSS hematuria (95% of cases) • Microscopic hematuria with a pelvic fracture • No pelvic fracture + No gross hematuria excludes injury to bladder • What about pelvic # and microscopic hematuria? --> Do a retrograde CT cystography
Bladder Injury - Imaging • Retrograde cystography (either CR or CT) is imaging modality of choice • Very sensitive
Bladder Injury - Management • Contusions – conservative • Intra-peritoneal – operative repair • Extra-peritoneal – many are now managed non-operatively with an indwelling foley catheter, will usually heal spontaneously.
Ureteral Injury • Extremely rare, gunshot is most common • No reliable Phx findings! Usually a retrograde diagnosis • Urinalysis is normal 25% of the time, do not rely on it • Being suspicious for it is the only way you will catch it • Imaging: Delayed CT with IV contrast • Management: Requires OR
Renal Injury • 90% blunt trauma, 10% penetrating • Again, relax. ‘Something else will kill them’ (less than 0.1% of trauma death)
Hematuria and Renal Injury • Poor correlation with degree of injury • Microscopic hematuria on its own is not a concern. Repeat urinalysis in 3 weeks • You should image if the following: • Microscopic hematuria with shock • GROSS hematuria • Rapid deceleration without hematuria or shock (rare, but important) • Penetrating trauma in the region
Renal Imaging • CT with IV contrast is 90-100% SENS • Remember, FAST ultrasound is not good for solid organ injury, do not use it in this setting • Formal ultrasound not as sensitive as CT
Renal Injury - Management • If no ‘rapid’ deceleration mechanism (how rapid?) and no gross hematuria, can d/c home with f/u urinalysis • Grade I and II injuries non-operative. ‘Bed rest’ until gross hematuria clears. • Grade III and up decision point for urology
Ask Me For References • Questions?