Aerobic Gram Positive Bacilli
720 likes | 916 Vues
Aerobic Gram Positive Bacilli. Bacillus. Introduction. The genus Bacillus includes gram positive, aerobic, spore-forming, rod shaped organisms. The diameter of the organism is 1 X 3-5µm

Aerobic Gram Positive Bacilli
E N D
Presentation Transcript
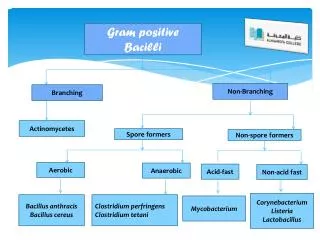
Aerobic Gram Positive Bacilli Bacillus
Introduction • The genus Bacillus includes gram positive, aerobic, spore-forming, rod shaped organisms. • The diameter of the organism is 1 X 3-5µm • They are arranged as single or paired bacilli in clinical specimens and as long serpentine chains or clumps in cultures. • It is ubiquitous in nature and B. species are well known in the food industries as troublesome spoilage organisms.
A large number of species belong to the genus that infect invertebrates but Bacillus anthracis, the agent of anthrax, is the only obligate Bacillus pathogen in vertebrates. • They produce a variety of enzymes and other metabolites during growth including the antibiotics bacitracin and polymyxin.
Bacillus anthracis • The causative agent of anthrax. • Pathogenesis depends on two plasmid encoded virulence factors: The Capsule - A prominent poly D- glutamic acid capsule which is observed in clinical specimens but is not produced in vitro. - It is antiphagocytic but is a poor immunogen and antibodies produced against it are not protective.
Toxin - It consists of three antigenically distinct heat labile proteins; protective antigen, lethal factor and edema factor. - None of the components is active alone, but the combination of protective antigen and either lethal factor or edema factor is active (toxic). - Protective immunity requires antibodies against components of the toxin, primarily the protective antigen.
Clinical Syndromes • Bacillus anthracis is an organism found in soil and on vegetation. • Anthrax is a disease of herbivores and humans are accidentally infected by exposure to infected animals or animal products. • Humans acquire disease by one of three routes, inoculation leading to cutaneous anthrax, inhalation leading to pulmonary anthrax and ingestion leading to gastrointestinal anthrax.
Approximately 95% of anthrax infections are due to the inoculation of spores through exposed skin surfaces either from contaminated soil or infected animal products such as hides, hair or wool. • Inhalation anthrax (wool sorters disease) results from inhalation of spores during processing of hair or wool. • Ingestion anthrax is very rare in humans but ingestion is a common route of infection in herbivores. • Person to person transmission does not occur.
Cutaneous Anthrax • It usually occurs through contamination of a cut wound or abrasion although in some countries biting flies may also transmit the disease. • After 2 to 3 days of incubation a small pimple or papule appears at the site of entry. A surrounding ring of vesicles develops, the central papule ulcerates, dries and blackens to form the characteristic eschar. • The lesion is painless and is surrounded by marked edema. • Lesions on the face or neck are dangerous and fulminating septicemia may develop in 20% of cases.
Pulmonary Anthrax • Inhaled spores are transported by alveolar macrophages to the mediastinal lymph nodes where they germinate and multiply to initiate systemic disease. • It may initially mimic a viral respiratory illness and then rapidly progresses to a diffuse pulmonary involvement leading to respiratory failure. • It is highly fatal (> 95%) because it is not suspected until the course is irreversible.
Gastrointestinal Anthrax • Very rare with varied clinical presentation (mesenteric adenopathy, hemorrhage and ascites) and high mortality rate (95%). • The organism probably invades the mucosa through a preexisting lesion and spreads to the lymphatic system. • Symptoms prior to fulminant systemic anthrax may be absent or mild. • During this phase the organism is multiplying and producing toxin in the regional lymph nodes and spleen.
Released toxin causes breakdown of organs probably of the spleen in particular. • This causes the sudden onset of hyperacute illness with dyspnea, cyanosis, high fever and disorientation which progress in a few hours to shock, coma and death. • This phase is marked by a high grade bacteremia but blood culture is not always positive.
Clinical diagnosis of anthrax is confirmed by directly visualizing or culturing the anthrax bacilli. • Acellular vaccines for human use are available for individuals in high risk occupations (cell free filtrate of culture). • Bacillus anthracis is susceptible to penicillin and almost all other broad spectrum antibodies.
Anthrax - Diagnosis • Specimen • Aspirate or swab from cutaneous lesion • Blood • Sputum • Laboratory investigation • Gram stain • Culture • Identification of isolate
Other Diseases • In recent years, other B. species have been increasingly implicated in a wide range of infections. • They include abscesses, bacteremia/septicemia, wound and burn infections, ear infections, endocarditis, meningitis, ophthalmitis, osteomyelitis, peritonitis and respiratory and urinary tract infections. • Most of these are secondary infections in immuno -compromised patients and the species most commonly associated with these diseases are B. cereus, B. licheniformis and B. subtilis.
Bacillus cereus • Large, motile, saprophytic bacillus • Heat resistant spores • Preformed heat and acid stable toxin (Emetic syndrome) • Heat labile enterotoxin (Diarrhoeal disease) • Lab diagnosis – Demonstation of large number of bacilli in food
Food Poisoning • B. cereus causes food poisoning by virtue of toxin production. • Two forms of food poisoning: Diarrheal type (heat labile toxin). - Characterized by diarrhea and abdominal pain occurring 8-16 hours after consumption of contaminated food. - It is associated with a variety of foods including meat and vegetable dishes, sauces, pastas, deserts and dairy products
Emetic type (heat stable toxin) - Nausea and vomiting begin 1 to 5 hours after consumption of contaminated food. - Boiled rice that is held for prolonged periods at ambient temperature and then quickly fried before serving is the usual offender. - Dairy products may also be responsible.
Bacillus cereus clinical presentation Gastroenteritis EMETIC FORM DIARRHOEALFORM Incubation period > 6 hours Diarrhea Lasts 20-36 hours Incubation period < 6 hours Severe vomiting Lasts 8-10 hours
B. cereus cause panophthalmitis by an incompletely defined mechanism (necrotic toxin, cereolysin which is a potent hemolysin, and phosphlipase C which is a potent lecithinase). • It is a post traumatic disease which is rapidly progressive that almost universally ends in complete loss of light perception within 48 hours.
Corynebacteria • Gram-positive, non motile, club shaped pleomorphic bacilli that appear in short chains [(V or Y) configurations] or in clumps resembling Chinese letters. • Nonencapsulated, catalase positive, and oxidase negative • C. diphtheriae is fastidious while diphtheriods are not • They contain metachromatic granules (polymetaphosphate) which stain bluish purple with methylene blue.
There are both gram-positive and gram-negative species, although the majority of isolates are gram-positive. • Corynebacteria are aerobes or facultative anaerobes and generally grow slowly on enriched media. • Four distinct cultured types exist; gravis, intermedius, mitis and belfanti. • These variants (biotypes) have been classified on the basis of growth characteristics, biochemical reactions and severity of disease.
They colonize skin, upper respiratory tract, gastrointestinal tract and urogenital tract of humans. • The most important species is C. diphtheriae, the causative agent of diphtheria which causes disease by virtue of toxin production. • Diphtheria toxin is a very potent exotoxin that is lethal at doses as little as 100 to 150 ng /kg of body weight. .
Nontoxigenic (avirulent) C. diphtheriae are morphologically indistinguishable from the virulent (toxigenic) strains • It is now recognized that avirulent strains may be converted to the virulent phenotype following infection and lysogenization by one of a number of distinct corynebacteriophages that carry structural gene for diphtheria toxin. • Lysogenic conversion may occur in situ as well as in vitro.
Pathogenesis • In 1883 Klebs demonstrated that C. diphtheriae is the agent of diphtheria. • The pathogenesis of diphtheria is based upon two primary determinants: 1) The ability of a given strain to colonize in the nasopharyngeal cavity and/or on the skin 2) Its ability to produce the toxin.
Diphtheria Toxin • The regulation of diphtheria toxin gene expression is mediated by an iron-activated repressor which is encoded on the C. diphtheriae genome. • Activation of the repressor gene derepresses the tox gene and diphtheria toxin is synthesized and secreted into the culture medium at maximal rates.
It is composed of a single polypeptide chain of 535 amino acids which consists of 3 structural functional domains: • An N-terminal ADP- ribosyl transferase (catalytic domain) • A region which facilitates the delivery of the catalytic domain across the cell membrane (transmembrane domain). • The eukaryotic cell receptor binding domain.
Following mild digestion with trypsin and reduction under denaturing conditions, the toxin is cleaved into two polypeptide fragments (A and B). • Fragment A is the N-terminal containing the catalytic center for the ADP- ribosylation of elongation factor 2 (EF-2). • Fragment B (the C terminal) carries the transmembrane and receptor binding domain of the toxin. • One molecule can inactivate the whole factor.
The intoxication of eukaryotic cells by diphtheria toxin involves at least four distinct steps: • Binding of toxin to its cell surface receptor. • Clustering of charged receptors into coated pits and internalization of toxin by receptors mediated endocytosis. • Insertion of transmembrane domain into the membrane and delivery of the catalytic domain into the cytosol. • ADP- ribosylation of EF-2 irreversibly inhibiting protein synthesis.
Clinical Manifestations • Incubation of 2-6 days. • There are two types of clinical diphtheria; nasopharyngeal and cutaneous. • Diphtheria is most commonly an infection of the upper respiratory tract and causes fever, sore throat and malaise.
A thick, gray-green fibrin membrane, the pseudomembrane, often forms over the site(s) of infection as a result of the combined effects of bacterial growth, toxin production, necrosis of underlying tissue and the host immune response. • Symptoms of pharyngeal diphtheria vary from mild pharyngitis to hypoxia due to airway obstruction by the pseudomembrane.
The involvement of cervical lymph nodes may cause profound swelling of the neck (bull neck diphtheria). • The skin lesions in cutaneous diphtheria are usually covered by a gray-brown pseudomembrane. • Life-threatening systemic complications, principally loss of motor function (as difficulty in swallowing) and congestive heart failure may develop as a result of the action of diphtheria toxin on peripheral motor neurons and the myocardium.
Fully immune individual have asymptomatic colonization and partially immune persons develop a mild respiratory illness. • Disease is followed by long lasting immunity which is also achieved by immunization using diphtheria toxoid (protective level is 0.01 1U/ml)/ • Diagnosis: Requires demonstration of toxigenic C. Diphtheria in lesions (throat, nasopharynx, nose) by Elek test.
Laboratory diagnosis • Specimen: A throat swab • Culture: The swab is inoculated on Loeffler's serum medium and/or on blood tellurite agar aerobically at 37C for 24. • On Loeffler's serum medium: • Corynebacteria grow much more readily than other respiratory pathogens • Used to enhance the characteristic microscopical appearance of corynebacteria • The colonies of C. diphtheriae are small, granular, grey, smooth, and creamy with irregular edges
Cultural characteristics • On blood tellurite agar (McLeod's blood agar) • It is a selective medium for the isolation of C. diphtheriae (Potassium tellurite) • 3 biotypes of C. diphtheriae are characterized on BTA • i.e. Gravis, mitis and intermedius biotypes • The most severe disease is associated with the gravis biotype • Colony of gravis biotype is large, non-hemolytic & grey. • Colonies of mitis biotype are small, hemolytic and black • Colonies of intemedius biotype are intermediate in size, non-hemolytic with black center & grey margin.
Gram stain of C. diphtheriae C. diphtheriae on BTA
In Vitro: Elek’s Test • Principle: • It is a toxin/antitoxin reaction • Toxin production by C.diphtheriae can be demonstrated by a precipitation between exotoxin and diphtheria antitoxin • Procedure: • A strip of filter paper impregnated with diphtheria antitoxin is placed on the surface of serum agar • The organism is streaked at right angels to the filter paper • Incubate the plate at 37C for 48 hrs
Filter paper saturated with diphtheria antitoxin Lines of precipitations • Results: • After 48 hrs incubation, the antitoxin diffusing from filter paper strip and the toxigenic strains produce exotoxin, which diffuses and results in four precipitation lines radiating from intersection of the strip and the growth of organism Inoculated M.O. Positive Elek’s Test
Epidemiology • Worldwide distribution. • Incidence has dropped dramatically since the introduction of the vaccine. • Crowding and low immunity promote spread and it is maintained in the population by asymptomatic carriage in the oropharynx or on the skin of immune individuals. • Infections is acquired by direct (person-to-person) spread via respiratory droplets or skin contact.
30-60% of adults have antitoxin antibodies below the protective level and are at risk. • Epidemics in Russia; since 1994, 80.000 cases and 2000 deaths. • Immunity can be assessed by serology or the Shick test. • Control is based on immunization (adults should be reimmunized every 10 years)