Biomechanics of Shoulder Complex.
Biomechanics of Shoulder Complex. Prepared by: Dr. Faryal Zaidi MSPT(KMU), BSPT(UHS), T- dpt *(KMU). OBJECTIVES. At the end of this lecture students should be able to: Define different terms of biomechanics Identify different structures in shoulder complex

Biomechanics of Shoulder Complex.
E N D
Presentation Transcript
Biomechanics of Shoulder Complex. Prepared by:Dr. Faryal Zaidi MSPT(KMU), BSPT(UHS), T-dpt*(KMU)
OBJECTIVES At the end of this lecture students should be able to: • Define different terms of biomechanics • Identify different structures in shoulder complex • Explain kinetics and kinematics of shoulder joint • Describe different pathologies of shoulder complex
Biomechanics • The term biomechanics combines the prefix bio, meaning “life,” with the field of mechanics, which is the study of the actions of forces, (both internal muscle forces and external forces.) In biomechanics we analyze the mechanical aspects of living organisms.
Subdivisions • statics: study of systems in constant motion, (including zero motion) • dynamics: study of systems subject to acceleration • kinematics: study of the appearance or description of motion • kinetics: study of the actions of forces (Force can be thought of as a push or pull acting on a body.)
kinematics • What we visually observe of a body in motion is called the kinematics of the movement. Kinematics is the study of the size, sequencing, and timing of movement, without regard for the forces that cause or result from the motion. The kinematics of an exercise or a sport skill is known, more commonly, as form or technique.
Kinetics • Kinetics is the study of forces, including internal forces (muscle forces) and external forces (the forces of gravity).
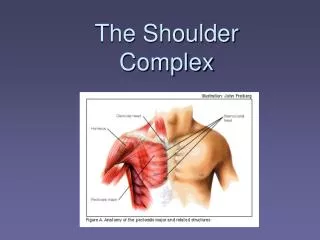
SHOULDER COMPLEX Five Functional Joints 1. Glenohumeral Joint 2. Subacromial 3. Scapulothroasic 4. Acromioclavicular 5. Sternoclavicular
SC JOINT Clavicle articulates with manubrium of the sternum • Weak bony structure but held by strong ligaments • Fibrocartilaginous disk between articulating surfaces • Shock absorber and helps prevent displacement forward • Clavicle permitted to move up and down, forward and backward and in rotation • Clavicle must elevate 40 degrees to allow upward rotation of scapula and thus shoulder abduction
SC JOINT • The only attachment of the upper extremity to axial skeleton • Plane synovial joint with degree of freedom 6, having joint capsule, joint disk and three major ligaments • Movement of the SC joint produces scapular movements, if it is fused the equal amount of movement will occur at AC joint
LIGAMENTS OF SC JOINT LIGAMENTS: • InterclavicularLig. • CostoclavicularLig. • Posterior Ligament Sternoclavicular
MOVEMENTS OF SC JOINT Movements in horizontal plane: • Protraction (30 degree)limited by costoclavicular and post. capsule • Retraction (30 degree) limited by costoclavicular and ant. capsule
MOVEMENTS OF SC JOINT • Elevation (48 degree) • limited by costoclavicular • Depression (less than15 degree) • limited by first rib Axial Rotation Ant. Rot. (very limited – 10 degree) Post. Rot. (50 degree)
AC JOINT • Lateral end of clavicle with acromion process of scapula • Weak joint and susceptible to sprain and separation • Joint capsule n two major ligaments and disk – present or absent
AC JOINT LIGAMENTS: • Coracoclavicular • Medial: Conoid • Lateral: Trapezoid • Acromioclavicular • Superior • Inferior • Coracoacromial: • Coracoids process to acromiom process • Closed packed position is when the humerus is abducted to 90 degree.
MOVEMENTS OF AC JOINT • Internal and external rotation • Bringing the glenoid fossa of the scapula anteromedially and posterolaterally, respectively • Anterior and posterior tiping or tilting • Ant. - acromion tipping forward and the inferior angle tipping backward • Post. - rotate the acromion backward and the inferior angle forward. • Upward and downward rotation • Upward rotation tilts the glenoid fossa upward and downward rotation is the opposite motion.
CORACOACROMIAL ARCH Arch over the GH joint formed by Coracoacromial arch,acromionand coracoid process • Sub acromial space: area in between CA arch and humeral head • Supraspinatus tendon, long head biceps tendon, and sub acromial bursa • Subject to irritation and inflammation as a result of excessive humeral head translation or impingement from repeated overhead activity
Structures Within Suprahumeral Space 1. Long head of biceps 2. Superior capsule 3. Supraspinatus tendon 4. Upper margins of subscapularis & infraspinatustendons 5. Subacromial bursa 6. Inferior surface of the A-C joint
SUBACROMIAL SPACE Clinical Relevance Avoidance of impingement during elevation of the arm requires • External rotation of humerus to clear greater tuberosity • Upward rotation of scapula to elevate lateral end of acromiom
SUBACROMIAL SPACE • Primary Impingement Structural stenosis of subacromial space • Secondary Impingement Functional stenosis of subacromial space due to abnormal arthrokinematics
Glenohumeral Joint Ball and socket, synovial joint in which round head of humerus articulates with shallow glenoid fossa of scapula • stabilized slightly by fibrocartilaginous rim called the Glenoid Labrum • Humeral head larger than glenoid fossa • At any point during elevation of shoulder only 25 to 30% of humeral head is in contact with glenoid Statically stabilized by labrum and capsular ligaments Dynamically stabilized by deltoid and rotator cuff muscles • Three degrees of freedom Stability provided by • Passive restraints • Active restraints
Glenoid Labrum • When the arms hang dependently at the side, the two articular surfaces of the GH joint have little contact. The majority of the time, the inferior surface of the humeral head rests on only a small inferior portion of the fossa. The total available articular • surface of the glenoid fossa is enhanced by an accessory structure, the glenoid labrum. This structure surrounds and is attached to the periphery of the glenoid fossa enhancing the depth or curvature of the fossa by approximately 50%. • the labrum was traditionally thought to be synoviumlined fibrocartilage, more recently it has been proposed that it is actually a redundant fold of dense fibrous connective tissue with little fibrocartilage other than at the attachment of the labrum to the periphery of the fossa. • The labrum superiorly is loosely attached, whereas the inferior portion is firmly attached and relatively immobile.Theglenoid labrum also serves as the attachment site for the glenohumeralligaments and the tendon of the long head of the biceps brachii.
GH CAPSULE • The entire GH joint is surrounded by a large, loose capsule that is taut superiorly and slack anteriorly and inferiorly in the resting position (arm dependent at the side).The capsular surface area is twice that of the humeral head.39 More than 2.5 cm of distraction of the head from the glenoid fossa is allowed in the loose-packed position. • The relative laxity of the GH capsule is necessary for the large excursion of joint surfaces but provides little stability without the reinforcement of ligaments and muscles. When the humerusis abducted and laterally rotated on the glenoid fossa, the capsule twists on itself and tightens, making abduction and lateral rotation the close-packed position for the GH joint
GH LIGAMENTS • SGHL • MGHL • IGHL • Anterior band • Posterior band • Axillary band