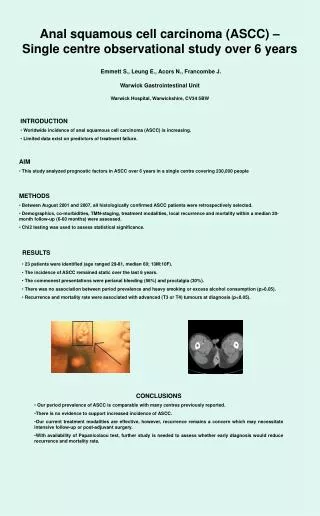
Download
1 / 21
220 likes | 547 Vues
High Incidence of Esophageal Squamous Cell Carcinoma in the Kalenjin Population of Kenya. Chris Huff, MD PGY-3. M.C. 54 yo female presents with worsening SOB and dry cough x 1 month. Also mild dysphagia with solids. Denies chest pain, orthopnea, PND, LE swelling.

E N D
High Incidence of Esophageal Squamous Cell Carcinoma in the Kalenjin Population of Kenya Chris Huff, MD PGY-3
M.C. • 54 yo female presents with worsening SOB and dry cough x 1 month. Also mild dysphagia with solids. • Denies chest pain, orthopnea, PND, LE swelling. • No fever, chills, night sweats, hemoptysis • PMH: none • Fam Hx: NC • Soc Hx: no toxic habits • Meds: none • All: NKDA
M.C. EXAM: Gen: mild resp distress VS: 36.8, P85, BP90/60, R26, 88% RA Heart: RRR, no m/r/g Lungs: coarse breath sounds throughout all lung fields bilaterally Abd: benign, no HSM Node: no palpable LAD Ext: warm, no edema
M.C. • HCT 32 • WBC 8 • Plt 250 • Creat 1.2 • Na+ 128 • HIV (-) • CXR – diffuse interstitial opacities bilat. with mediastinal LAD
M.C. Hospital Course: • Admitted to the medicine service and treated empirically with Rocephin, Azithromycin, and 4 drug TB therapy • Worsened over the next few days, so steroids and nebulizer initiated • On HD #5 sats 35% on 15L
M.C. • Patient transferred to the ICU with plan for intubation • Pt intubated and after inflation of the cuff, was discovered to have persistent air leak • Also stomach and chest both rising with bagging
M.C. • Patient was felt to most likely have tracheo-esophageal fistula (TEF) • Gen Surg consulted for EGD and cancer found in mid portion of esophagus with extension to the trachea, creating TEF • Pt made comfort care and expired 1 hr later from resp. failure
Esophageal SCC in Western Kenya • Epidemiology: - Most common cancer in Men and 3rd most common in women - Incidence 200 per 100,000 • Male to female ratio of 1.5 to 1 • Mean age at diagnosis 58.7 yrs • 90% is squamous cell
Esophageal SCC in Western Kenya • Tenwek Hospital Bomet Kenya - Retrospective Review of esophageal cancer diagnoses 1999-2007 - Esophageal cancer accounted for 914 (34%) of newly diagnosed cancers - 6.3% of pts </= to 30yo, 1% </= to 20yo Dis Esophagus. 2009 May 15.
Esophageal SCC in Western Kenya • Risk Factors: • Family history • EtOH and tobacco • Corn and Wheat Diet (2 main hypotheses) 1) Deficiency of A, C, E, selenium, zinc 2) Exposure to the corn mold Fusarium moniliforme Sheldon 3) Polycyclic Aromatic Hydrocarbons from food contaminated with smoke or soot
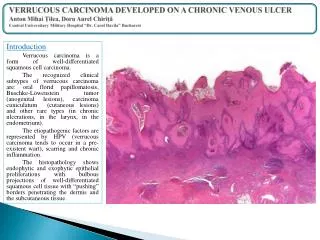
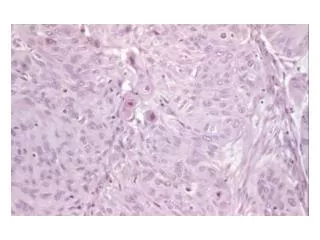
Esophageal SCC in Western Kenya • Pathophysiology: • Arises from polyps, plaques, or denuded epithelium • Usually occurs in the mid-esophagus • Early invasion of submucosa and extends in cephalad direction • Invades lymph nodes early b/c the lymphatics are located in the lamina propria
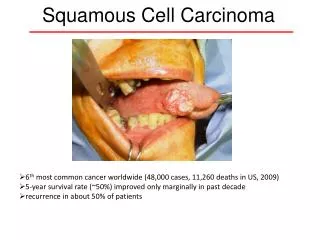
Esophageal SCC in Western Kenya • Clinical Manifestations: • Dysphagia and weight loss most common • Vomiting and chest pain • Iron deficiency anemia without melena • Respiratory symptoms if TEF develops
Esophageal SCC in Western Kenya • Tracheoesophageal Fistula: How rare? - European study in 2008 264 of 2113 patients with esophageal cancer were found to have a TEF • Incidence in Kenya unknown
Esophageal SCC in Western Kenya • Diagnosis of Esophageal Cancer: - Barium swallow can suggest, but need EGD with biopsy to make the diagnosis - On EGD can appear as plaque, stricture, ulceration, or mass - Diagnosis improves with number of biopsies taken: 1= 93%, 7=98%
Esophageal SCC in Western Kenya • Staging of Esophageal Cancer: - TNM criteria – 5 yr survival related to stage: I 60% II 31% III 20% IV 4%
Esophageal SCC in Western Kenya • Staging of Esophageal Cancer: - CT scan to evaluate for metastasis (M) - EUS for locoregional staging (T & N) - Possible PET to better eval for mets prior to surgery **EUS and PET not available in Western Kenya and staging CT often not performed because of financial reasons
Esophageal SCC in Western Kenya • Treatment: Depends on Stage - Neoadjuvant chemoradiation followed by surgery for stage I – IIIa - Cisplatin/5-FU chemo recommended - 60% unresectable at diagnosis - Chemoradiation - Palliative care (may include stenting)
Conclusions • Esophageal Cancer is common and occurs at an early age in Western Kenya • Risk factors are combination of genetic and environmental • Diagnosis made with EGD and biopsy • In remote areas of Kenya treatment limited to surgical resection vs palliative care
References • Balazs et al. Eur J Cardiothorac Surg 2008;34:1103-1107 • Parker et al. Frequent occurrence of esophageal cancer in young people in western Kenya Dis Esophagus. 2009 May 15 • Wakhisi et al. Esophageal cancer in north rift valley of Western Kenya. Afr Health Sci. 2005 Jun;5(2):157-63 • White et al. Esophageal Cancer: a common malignancy of young people in Bomet District, Kenya. Lancet. 2002 Aug 10;360(9331):462-3 • http://img.medscape.com/fullsize/migrated/423/508/mgi423508.fig6.jpg • www.freetalaba.com/.../index.php?t13243.html • http://www.gastrointestinalatlas.com/EsophagealCa2.jpg • Graham et al. Prospective evaluation of biopsy number in the diagnosis of esophageal and gastric carcinoma.Gastroenterology 1982 Feb;82(2):228-31 • Rationale of staging in cancer of the esophagus. In: International Trends in General Thoracic Surgery: Esophageal Cancer, vol 4, Delarue, N, Wilkins, EW, Wong, J Eds), CV Mosby, St Louis 1988. • Mallery, S, Van Dam, J. Increased rate of complete EUS staging of patients with esophageal cancer using the nonoptical, wire-guided echoendoscope. Gastrointest Endosc 1999; 50:53. • Bolton, JS, Fuhrman, GM, Richardson, WS. Esophageal resection for cancer. Surg Clin North Am 1998; 78:773.