Download
1 / 17
170 likes | 389 Vues
Immunotherapy (Cancer therapy with T-Cells). Sania Munir 12-10235 BIOT- 412. Cancer Therapy with T-Cells. T- cells Cytotoxic -T-lymphocytes (CTL) Are designed to destroy the target cells Video!!. Using a Bispecific Monoclonal Antibody.

E N D
Immunotherapy(Cancer therapy with T-Cells) Sania Munir 12-10235 BIOT- 412
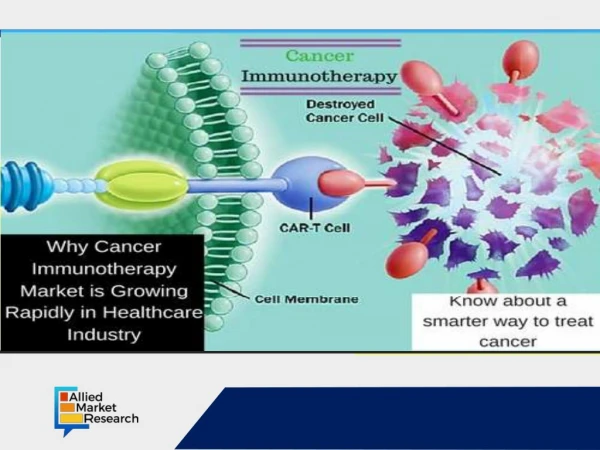
Cancer Therapy with T-Cells • T- cells • Cytotoxic-T-lymphocytes (CTL) • Are designed to destroy the target cells Video!!
Using a Bispecific Monoclonal Antibody • Blinatumomab is a synthetic monoclonal antibody, carries binding sites. • One arm binds to CD19 (B-Cells lymphomas) • Other arm binds to CD3, a cell surface molecule on T cells (CTLs) • Form a bridge b/w CD3 and CD19, attaches T-cells to B-cells and activate T-cells to kill B-cells.
Allografts of T-Cells • After total destruction of the pateint’s own white blood cells (myeloablative conditioning) • To cure leukemia (and some other cancers)→high doses of chemotherapy and radiation →patient's bone marrow is destroyed. • If the patient is to survive the treatment, he or she must be given a transplant of hematopoietic stem cells.
The stem cells can be • an autograft; that is, from bone marrow harvested from the patient and stored before treatment begins. • an allograft; that is, cells harvested from another person, usually a family member sharing the same major histocompatibility molecules.
Allografted hematopoietic stem cells also sometimes fail to cure. But….??? • graft-versus-leukemia effect. • Most of the donor T cells are probably attacking normal cell surface molecules, not tumor-specific ones. • The patient may also suffer from graft-versus-host disease (GVHD).
After Non-myeloablative Conditioning • The patient is treated to kill some bone marrow cells. • Instead of using high doses of radiation to the entire body and chemotherapy, only the lymphoid organs are irradiated. • Antithymocyte globulin can also be given. • Even though this leaves some cancer cells, it makes it possible for allogeneic bone marrow stem cells to take up long-term residence in the recipient.
This is followed by an infusion of T cells from the same donor. • Once again they will also attack normal cells of the recipient usually causing graft-versus-host disease (GVHD). Butthis it wouldbe milder than that following myeloablative conditioning — perhaps because repeated small doses of radiation favors the survival of natural killer (NK) cells, and these appear to protect against GVHD.
Autografts of T cells: Tumor-Infiltrating Lymphocytes (TIL) The procedure: • Isolate T cells — both CD4+and CD8+ from samples of the tumor (melanoma) • In-vitro testing • Grow large numbers of them in culture (using the powerful T-cell growth factor IL-2) • Treat the patient with modest doses of cytotoxic drugs to reduce — but not destroy — the bone marrow • Reintroduce the mix of Th cells (CD4+) and CTL (CD8+) into the patient (along with IL-2).
The results: • The infused cells usually took up long-term residence. • In 10 of 13 patients, their melanoma cells — including all metastases — regressed either partially or completely. • In a few cases, the TIL seemed to be reacting to tumor-specific antigens, but in most the target seems to have been antigens expressed by all melanin-containing cells. Evidence: • Four patients lost normal melanocytes from their skin leaving white patches. • One patient developed inflammation of the uvea. Video!!
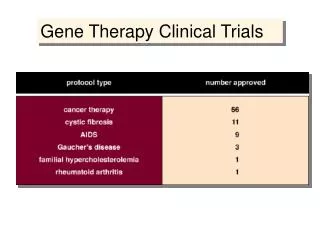
Gene Therapy: Autografts of genetically-modified T cells • On April 20, 2006, the Rosenberg group reported some success with melanoma patients using a modification of the TIL procedure. • The patient's T cells were removed and treated with a retroviral vector containing the αβ TCR specific for a melanoma antigen. • Large numbers of these were grown in culture. • After partial myeloablative conditioning, the genetically-modified lymphocytes were infused into the patient.
Cont. • This application of gene therapy succeeded in eliminating the metastases and providing a disease-free period of two years in two patients. • Video!!
Autografts of a clone of tumor-antigen-specific T cells • The 19 June 2008 issue of the New England Journal of Medicine (Naomi Hunderet al) carried a report describing the successful treatment of a man with metastasized melanoma using his own T cells. The procedure: • His leukocytes were harvested and a mixed culture was prepared containing • antigen-presentingdendritic cells. • a peptide from the antigenNY-ESO-1. • The patient's own T cells. • After repeated stimulation with the antigen, responding cells wereclonedbylimiting dilution.
One (of four) antigen-reactive cells was then expanded in culture until5 billion (5 x 109) identical anti-NY-ESO-1 CD4+T cells were available to infuse into the patient. The result: • Complete regression of each metastatic clump of melanoma cells, and the patient has remained free of this lethal cancer for two years since this treatment.
“One swallow does not make a summer”, but this result give hope that in time immunotherapy will become an effective weapon against cancer.