Download
1 / 109
1.09k likes | 1.56k Vues
Inflammatory Disorders. Updated Fall 2012 by Renee Redman From the notes of Nancy Jenkins. Overview of Today’s Lecture. A & P Review Endocarditis- infection of the endocardial surface of the heart Myocarditis- a focal or diffuse inflammation of the myocardium

E N D
Inflammatory Disorders Updated Fall 2012 by Renee Redman From the notes of Nancy Jenkins
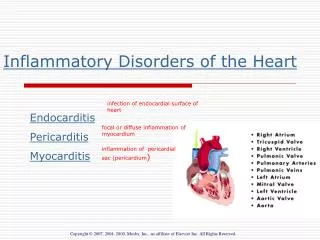
Overview of Today’s Lecture • A & P Review • Endocarditis- infection of the endocardial surface of the heart • Myocarditis- a focal or diffuse inflammation of the myocardium • Pericarditis- inflammation of the pericardial sac (the pericardium)
A- Aortic Valve B- Mitral Valve D- Tricuspid Valve - Pulmonary Valve
Anatomy and Physiology Review Blood enters the right atrium and moves through the _______ into the right ventricle. Blood then moves from the right ventricle into the pulmonary artery via the _________. A- Aortic Valve B- Mitral Valve C- Pulmonary Valve D- Tricuspid Valve
Anatamy and Physiology Review (Cont’d) • After entering the left atrium via the pulmonary veins, blood moves through the _____ into the left ventricle. • Finally, it travels through the _____ and out of the heart. A- Aortic Valve B- Mitral Valve C- Pulmonary Valve D- Tricuspid Valve
Infective Endocarditis • Infection of the inner layer of the heart • Usually affects the cardiac valves • Was almost always fatal until • development of penicillin • Around 15,000 cases diagnosed • annually in the U.S.
Causative Organisms • Causative organism –often bacterial • Streptococcus viridans • Staphylococcus aureus • Other Etiologies • Viruses- Coxsackie B • Fungi – Candida alibcans
Etiology and Pathophysiology • Occurs when blood turbulence within heart allows causative agent to infect previously damaged valves or other endothelial surfaces
Etiology and Pathophysiology • Vegetation - • Fibrin, leukocytes, platelets, and microbes • Adhere to the valve or endocardium • Embolization of portions of vegetation into circulation • 50% of patients with IE will have systemic embolization
Endocarditis • Infection of the innermost layers of the heart • May occur in people with congenital and valvular heart disease • May occur in people with a history of rheumatic heart disease • May occur in people with normal valves with increased amounts of bacteria
Etiology/Pathophysiology • Endocarditis • When valve damaged, blood is slowed down and forms a clot. • Bacteria get into blood stream • Bacterial or fungal vegetative growths deposit on normal or abnormal heart valves
Classifications of Endocarditis • Acute Infective Endocarditis • Abrupt onset • Rapid course • Staph Aureus • Subacute Infective Endocarditis SBE • Gradual onset • Systemic manifestations • Prosthetic Valve Endocarditis • Or named by cause (IVDA endocarditis, Fungal IE)
Risk Factors- endocarditis • Hx of rheumatic fever or damaged heart valve- less common now (20% of cases) • Prior history of endocarditis • Aging (50% associated with aortic stenosis) • Invasive procedures- (introduce bacteria into blood stream) (surgery, dental, etc) • Permanent Central Venous Access- MRSA • IV drug users • Valve replacements • Renal dialysis
Nursing Assessment • Subjective Data • History of valvular, congenital, or syphilitic cardiac disease • Previous endocarditis • Staph or strep infection • Immunosuppressive therapy • Recent surgeries and procedures
Nursing Assessment • Functional health patterns • IV drug abuse • Alcohol abuse
Nursing Assessment • Nonspecific Clinical Manifestations • Weight changes • Chills • Low grade fever in 90% patients • Malaise
Nursing Assessment • Diaphoresis • Bloody urine • Exercise intolerance • Generalized weakness • Fatigue • Cough • Headache
Nursing Assessment • Dyspnea on exertion • Night sweats • Chest, back, abdominal pain • Also consider s/s related to embolization to specific organ • New or changing heart murmur
Collaborative Care • Fungal and prosthetic valve endocarditis • Responds poorly to antibiotics • Valve replacement is adjunct procedure
Assesment endocarditis • Infection and emboli • Emboli-spleen most often affected (splenectomy) • Osler’s nodes- painful, red or purple pea-sized lesions on toes and fingertips • Splinter hemorrhages- black longitudinal streaks on nail beds • Janeway lesions- flat, painless, small, red spots on palms and soles • Roth spots- hemorrhagic retinal lesions • Murmur- most have murmurs • T above 101(blood cultures) and low-grade • Chills • Anorexia • Fatigue
Splinter hemorrhage • small areas of bleeding under the fingernails or toenails. • due to damage to capillaries by small clots
Janeway Lesions • flat, painless red spots on palms and soles
Osler’s Nodes • Painful, pea-size, red or purple lesions • On finger tips or toes Roth spots Osler’s nodes
Roth’s Spots • hemorrhagic retinal lesions
Clinical Manifestations • Murmur in most patients • Heart failure in up to 80% with aortic valve endocarditis • Manifestations secondary to embolism Heart Sounds Assessment Video
Auscultating Heart Sounds • The aortic area or right sternal border (RSB) is at the right 2nd intercostal space, just under and to the right of the angle of Louis (sternal angle) • The pulmonic area or left upper sternal border (LUSB) is at the left 2 nd intercostal space • The tricuspid area or left lower sternal border (LLSB) is at the left fifth intercostal space • The mitral area or apex is at the PMI -- the 5th intercostal space in midclavicular line
Past Medical History • Recent surgeries or procedures • Cardiac Cath,dental, urologocial, gynecological (including vaginal or c-section deliveries) Hx of IV drug use Central line placement Dialysis Infections (recent UTI, URI or skin infection) Immunosuppression
Diagnostic Tests • Blood Cultures- most likely positive unless recent antibiotic tx • Echocardiogram-TEE best- see vegetations • Other- WBC with differential, CBC,ESR, serum creatinine,CXR, and EKG
Major Diagnostic Criteria • Have at least two: • Positive blood culture • New or changed murmur • Echo positive for vegetation or mass • Could have: • CXR shows cardiomegaly • EKG with conduction A-V block
Medications • Antibiotics • IV for 4-8 weeks • Monitor peaks and troughs of certain drugs • Monitor BUN and Creatinine. • Evaluate effectiveness of treatment with repeated blood cultures. • Unclear of success of oral antibiotics
Additional Treatment • Fungal infections- poor responsive to drug therapy • May require valve replacement • Relapses are common • Bedrest usually not indicated unless febrile, HF or other complications
Nursing Diagnoses • Decreased cardiac output r/t valve insufficiency and altered rhythm • Activity intolerance r/t alternation in o2 transport system secondary to valve dysfunction • Hyperthermia r/t infection of endocardium • Risk for Ineffective Tissue Perfusion-emboli • Ineffective Health Maintenance
Complications • Emboli (50% incidence) • Right side- pulmonary emboli (esp. with IV drug abuse) • Left side-brain, spleen, heart, limbs, etc • CHF-check edema, rales, VS • Arrhythmias- A-fib, conduction blocks • Death .
Treatment Goal • Return to baseline cardiac function • ADL’s without fatigue • Prevent recurrence
Prevention • Eliminate risk factors • Patient teaching
Risk Stratisfication for IE High Risk- • Mechanical prosthetic heart valve • Natural prosthetic heart valve • Prior infective endocardititis • Valve repair with prosthetic material • Most congenital heart diseases Moderate Risk- • Valve repair without prosthetic material • Hypertrophic cardiomyopathy • Mitral valve prolapse with regurgitation • Acquired valvular dysfunction Low Risk- • Innocent heart murmurs • Mitral valve prolapse without regurgitation • Coronary artery disease • People with pacemakers/ defibrillators • Prophylactic antibiotics are generally recommended only for people in the “High Risk” category