Coding Conundrums
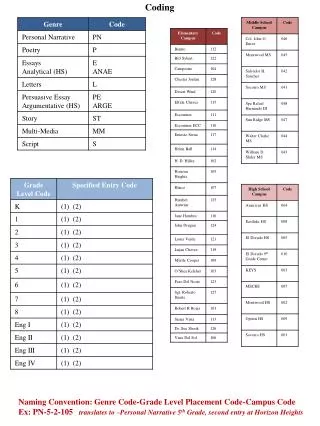
Coding Conundrums. Presented by Lori Dafoe, CPC & Marisa Clauson, CPC. Family Visits CPT Assistant Archives - Evaluation and Management (Q&A) (March 2013), page 13.


Coding Conundrums
E N D
Presentation Transcript
Coding Conundrums Presented by Lori Dafoe, CPC & Marisa Clauson, CPC
Family VisitsCPT Assistant Archives - Evaluation and Management (Q&A) (March 2013), page 13 • Assuming the physician wants to report the E/M service based on time with non-face-to-face patient contact, is it appropriate to report an office visit code (99211-99215) when the patient is not present? For example, the family of a stroke patient comes in to discuss the patient's care with the physician, while the patient is left at home.
Family Visits • Yes. The evaluation and management (E/M) services guidelines on page 8 of the 2013 CPT Professional Edition codebook state, "Face-to-face time (office and other outpatient visits and office consultations): For coding purposes, face-to-face time for these services is defined as only that time spent face-to-face with the patient and/or family. This includes the time spent performing such tasks as obtaining a history, performing an examination, and counseling the patient." • When counseling and/or coordination of care dominates (ie, more than 50%) the encounter with the patient and/or the patient's family (face-to-face time in the office or other outpatient setting or floor/unit time in the hospital or nursing facility), then time shall be considered the key or controlling factor to qualify for a particular level of E/M service. This includes time spent with parties, who have assumed responsibility for the care of the patient or decision making regardless if they are family members (eg, foster parents, person acting in loco parentis, legal guardian). The extent of counseling and/or coordination of care and the time spent performing this function must be documented in the patient's medical record. Although this reporting method reflects the intent of CPT coding, third-party payers may request that these services be reported differently.
Allergy Injection • Physician is out of the office. Patient presents for an allergy injection. • Can the nurse give it/bill for it (CPT 95115-95117)?
Allergy Injection • The nurse can technically give the injection in conjunction with state guidelines. Malpractice carriers would recommend that the physician be present. • “Incident To” guidelines mandate that a supervising provider be present in order to bill for a service that requires supervision.
Nurse Phone Call • Patient calls in for protime results. The nurse reviews all information including review of systems over the phone and gives instructions on adjusting meds and further testing. At least 10 minutes is spent on the call. • Can you bill a nurse visit (CPT 99211) for the phone call?
Nurse Phone Call • NO, 99211 would not be appropriate. Medicare requires that all E&M services be “face-to-face”. • Other carriers, may allow payment. 99441‑99443Telephone evaluation and management service provided by a physician to an established patient, parent, or guardian not originating from a related E/M service provided within the previous 7 days nor leading to an E/M service or procedure within the next 24 hours or soonest available appointment
CPT Assistant Archives - Evaluation and Management (Q&A) (March 2013) • If an OB/GYN physician was unable to perform a pelvic examination and pap smear during a preventive medicine evaluation and management (E/M) service and performed the pelvic examination and pap smear on a date subsequent to the preventive medicine E/M service visit, would it be appropriate to separately report for the subsequent visit?
Pap & Pelvic: AMA Comment, CPT Assistant Archives - Evaluation and Management Services (August 2004), page 10c • NO. The appropriate preventive medicine E/M service code should be reported for the first visit. As a pelvic examination and pap smear are considered part of a comprehensive OB/GYN preventive medicine E/M service, no additional reporting is necessary for the pelvic examination and pap smear performed on the subsequent date.
Breast & Pelvic Exam • Whenever the provider documents a that the breast and pelvic areas were examined, coders should automatically assign HCPC G0101.
G-Code for Breast & Pelvic Exam • FALSE. According to a Centers for Medicare & Medicaid Services (CMS) Medicare Learning Network product, G0101 is payable under the physician fee schedule when at least seven of the following 11 elements are included in the exam: • Inspection and palpation of breasts for masses or lumps, tenderness, symmetry, or nipple discharge • Digital rectal examination including sphincter tone, presence of hemorrhoids, and rectal masses • External genitalia (for example, general appearance, hair distribution, or lesions) • Urethral meatus (for example, size, location, lesions, or prolapse); • Urethra (for example, masses, tenderness, or scarring) • Bladder (for example, fullness, masses, or tenderness) • Vagina (for example, general appearance, estrogen effect, discharge, lesions, pelvic support, cystocele, or rectocele) • Cervix (for example, general appearance, lesions or discharge) • Uterus (for example, size, contour, position, mobility, tenderness, consistency, descent, or support) • Adnexa/parametria(for example, masses, tenderness, organomegaly, or nodularity) • Anus and perineum • In reviewing this issue, the ACOG Health Economics and Coding Committee determined that G0101 should be covered if the documentation notes the absence of the breast(s), cervix, uterus, fallopian tube(s), and/or ovary(s).
CPT Assistant Archives - Reporting of Cutaneous Excision Pending Pathology (May 2012) • If the provider is unsure whether the lesion is benign or malignant, coders should choose the correct CPT procedure code that relates to the manner in which the lesion was approached rather than the final pathologic diagnosis, since the CPT code should reflect the knowledge, skill, time, and effort that the physician invested in the excision of the lesion.
Reporting of Cutaneous Excision Pending Pathology • FALSE. This WAS the instruction given by CPT in 1996 & 2000; however, in May 2012, this guideline was updated. • In general, the selection of the appropriate excision code is determined by three parameters: location, maximum excised diameter (which includes the margin), and lesion type (ie, benign or malignant). When the lesion is clearly benign (eg, cyst, lipoma, prior biopsy of benign neoplasm), the excision can be coded as benign at the time of surgery (11400-11471). When there is a prior biopsy showing malignancy, the excision can be coded as malignant at the time of surgery (11600-11646). • Coding excision of a cutaneous lesion pending pathology (eg, lesion of unspecified behavior) as malignant before pathology is available could result in incorrect coding if the lesion is found to be benign on histopathologic examination. Therefore, if the lesion is not clearly benign or malignant, coding and billing should be delayed until the pathology has been confirmed. ♦
Preoperative Visits CPT Assistant Archives - Coding Clarification (May 2009), pages 9-10 • Pre-operative visits by the surgeon are always billable, as long as they occur prior to the start of the global period.
Preoperative Visits • FALSE. If the decision for surgery occurs the day of or day before the major procedure and includes the preoperative evaluation and management (E/M) services, then this visit is separately reportable. Modifier 57, Decision for Surgery, is appended to the E/M code to indicate this is the decision- making service, not the history and physical (H&P) alone). If the surgeon sees a patient and makes a decision for surgery and then the patient returns for a visit where the intent of the visit is the preoperative H&P, and this service occurs in the interval between the decision making visit and the day of surgery, regardless of when the visit occurs (1 day, 3 days, or 2 weeks), the visit is not separately billable as it is included in the surgical package. • Example: The surgeon sees the patient on March 1 and makes a decision for surgery. Surgery is scheduled for April 1. The patient returns to the office on March 27 for the H&P, consent signing, and to ask and clarify additional questions. This visit on March 27 is not billable, as it is the preoperative H&P visit and is included in the surgical package.
CPT Assistant Archives - Coding Brief: Immunization Administration (90460, 90461) (July 2012), page 7 • This service should only be billed when the counseling is provided by the physician or a registered nurse.
Immunization Administration & Counseling (90460, 90461) • FALSE. Codes 90460 and 90461 are reported only when the physician or qualified health care professional provides face-to-face counseling to the patient and/or the patient's family during the administration of a vaccine. The term "qualified health care professional" includes registered nurse practitioners and physician assistants and these codes may not be reported when other types of office clinical staff (eg, registered nurses or other office staff) provide the counseling and immunization administration.
CPT Assistant Archives - Coding Brief: Immunization Administration (90460, 90461) (July 2012), page 12 • CPT 90460 may only be reported once per encounter, as there can only be ONE initial immunization administration.
Immunization Administration & Counseling (90460, 90461) • FALSE. Code 90460 encompasses the delivery of either a single-component vaccine product, which provides protection for a single disease (eg, hepatitis B), or of the first component of a multiple-component vaccine product (ie, a combination vaccine), which provides protection for multiple diseases (eg, diptheria-tetanus-pertussis, hepatitis B, inactivated poliovirus vaccine [DTaP-HepB-IPV]). Code 90461 is reported for each additional component of a multiple-component vaccine beyond the first component. If a patient were to receive both types of the vaccines in the example, the administration code, 90460, would be reported twice.
Immunization Administration & Counseling (90460, 90461) - EXAMPLE To illustrate, the list of codes that would be reported for a 2-month-old infant based on the current immunization schedule is as follows:
Evaluation & Management • None of the 1997 documentation guidelines can be used in conjunction with 1995 documentation guidelines. • http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/Downloads/EM-FAQ-1995-1997.pdf
Evaluation & Management • FALSE. Effective Sept. 10, the CMS allows physicians to use the 1997 DG for an extended history of present illness (HPI) with the other elements of the 1995 DG to document an E/M service. As a result, “the status of three or more chronic conditions” qualifies as an Extended HPI for either set of DGs. • The revised guideline is presented as a Question and Answer on the CMS website: FAQ on 1995 & 1997 Documentation Guidelines for Evaluation & Management Services. • Q. Can a provider use both the 1995 and 1997 Documentation Guidelines for Evaluation and Management Services to document their choice of evaluation and management HCPCS code? • A. For billing Medicare, a provider may choose either version of the documentation guidelines, not a combination of the two, to document a patient encounter. However, beginning for services performed on or after September 10, 2013 physicians may use the 1997 documentation guidelines for an extended history of present illness along with other elements from the 1995 guidelines to document an evaluation and management service.
HPI Documentation • Does the provider have to document the HPI (history of present illness)?
HPI Documentation • GOOD QUESTION! • 1995 & 1997 Documentation guidelines state that the ROS and/or PFSH may be recorded by ancillary staff or on a form completed by the patient. To document that the physician reviewed the information, there must be a notation supplementing or confirming the information recorded by others. • Because the DG’s do not specifically state the HPI can be documented by ancillary staff, it is assumed that the provider must do this. However, the guidelines themselves DO NOT state this!
HPI Documentation - Noridian • Noridian’s E&M Clarification posted on 05/21/2007 indicates their expectation is that the provider will gather and record this information. • https://www.noridianmedicare.com/cgi-bin/coranto/viewnews.cgi?id=EEZAZlkyFyxzeFsPmT&tmpl=part_b_viewnews&style=part_ab_viewnews
https://www.noridianmedicare.com/cgi-bin/coranto/viewnews.cgi?id=EEZAZlkyFyxzeFsPmT&tmpl=part_b_viewnews&style=part_ab_viewnewshttps://www.noridianmedicare.com/cgi-bin/coranto/viewnews.cgi?id=EEZAZlkyFyxzeFsPmT&tmpl=part_b_viewnews&style=part_ab_viewnews
Documentation Guidelines, E/M Documentation When History Is Not Available (Q&A), January 1998, page 10 • Documenting E/M services and unresponsive and comatose patients. If the physician cannot obtain the history due to the patient's condition but does a comprehensive exam and the medical decision making is of high complexity, is this reported as a level three or not, since the history was not obtained (even though the reason he couldn't perform the history is documented)?
E/M When History Is Not Available AMA Comment • In those circumstances when the patient's nature of illness/injury does not lend itself to eliciting a history nor is it available from either a SNF or other hospital transfer sheet, the patient, family, significant other, or other source, or by performing a comprehensive examination, the physician should document in the medical record the circumstances which precluded obtaining this information or from doing the comprehensive examination. This shows a good faith effort on the part of the physician. The July 1997 edition of the CPT Assistant, page 5, A. Documentation of History, second column, second DG bullet states: • DG "If the physician is unable to obtain a history from the patient or other source the record should describe the patient's condition or other circumstance which precludes obtaining a history."
CPT Assistant Archives - Surgery: Digestive System (June 2006), page 16c • Is it appropriate to report CPT code 45915, Removal of fecal impaction or foreign body (separate procedure) under anesthesia, when conscious sedation is used?
Digestive System • NO. CPT code 45915 is intended to be reported for fecal impaction or foreign body removals only when performed under general anesthesia. The CPT code descriptors that include the phrase "requiring anesthesia" or "under anesthesia" indicate that the work involved in that specific procedure requires the use of general anesthesia; therefore, it would not be appropriate to report code 45915 if general anesthesia is not provided. Fecal impaction or foreign body removal performed with other anesthetics is considered inclusive to the appropriate evaluation and management service code.
CPT Assistant Archives - Surgery: Auditory System (July 2005), page 14 • Cerumen removal can only be billed if the documentation records an impaction, instrumentation is used, and it is performed by a physician.
Auditory System • CORRECT. Removing wax that is not impacted does not warrant the reporting of CPT code 69210. Rather, that work would appropriately be captured by an evaluation and management (E/M) code regardless of how it is removed. If, however, the wax is truly impacted, then its removal should be reported with 69210 if performed by a physician using at minimum an otoscope and instruments such as wax curettes or, in the case of many otolaryngologists, with an operating microscope and suction plus specific ear instruments (eg, cup forceps, right angles). Accompanying documentation should indicate the time, effort, and equipment required to provide the service.
National Drug Codes • When there is a 10 digit number listed on the drug insert, you should always add a “0” at the very beginning of the code to make it the 1 digit number that is required.
National Drug Codes • FALSE! • There are 3 segments to an NDC number that identifies the labeler, product and trade package size. Each segment is divided into sets of 5-4-2. • If the NDC# from the supplier is only 10 digits long, you will need to add a “0”, but it can be added in front of any of the digit number sets.
National Drug Codes • The first segment indicates the labeler code and is 4 or 5 digits long. • The second segment indicates the product and specifies the strength, dosage and formulation. It is 3 or 4 digits long. • The third segments is the package segment that identifies the package form and sizes. It consists of 1 or 2 digits.
National Drug Codes • For example: 5……4 …2 XXXX-XXXX-XX = 0XXXX-XXXX-XX XXXXX-XXX-XX = XXXXX-0XXX-XX XXXXX-XXXX-X = XXXXX-XXXX-0X
FDA-Food and Drug Administration NDC Website http://www.accessdata.fda.gov/scripts/cder/ndc/default.cfm Using our 5-4-2 formula, where would the “0” need to be inserted for this drug?
RAC Audits • When you have a redetermination for the RA (or any other post pay audit contractor), you cannot file a claim determination if it is over one year old. • Example: RAC audit indicates New Patient Visit was billed in error. Claim is from 2010. Since the initial visit date is over one year old, you must return the money and cannot re-bill a corrected claim for an established patient visit.
RAC Audits • FALSE! • You should not bill a corrected claim, but instead use the appeal process. • Make sure to mark the RA box on the interactive Redetermination, so that timely filing can be waived. Providers have 120 days from the initial demand letter to submit the redetermination.
Established Patient Visit? • If a physician has provided an interpretation for a study at the hospital, and then sees the patient in the office for the first time, this should be billed as an Established Patient Visit.
Established Patient Visit? • FALSE: • The guidelines state the service is within the past 3 years by the same provider or by the same specialty, within the same group. This guideline is explained in • http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c12.pdf Section 30.6.7A. • Exception: The interpretation of a diagnostic test, x-ray reading or EKG, etc., without an E/M or other face-to-face service does not affect the designation of a new patient.