Nerve Blocks
Nerve Blocks. Denise Ammon T4 Anesthesia 2/23/12. Brachial Plexus. Anatomy. Union of the anterior primary divisions of C5-8 and the T1 nerve. C4 and T2 may contribute as well. Roots Trunks Divisions Cords Terminal nerves (branches). “ Robert Taylor Drinks Cold Beer ”.


Nerve Blocks
E N D
Presentation Transcript
Nerve Blocks Denise Ammon T4 Anesthesia 2/23/12
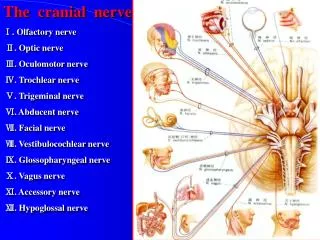
Anatomy • Union of the anterior primary divisions of C5-8 and the T1 nerve. • C4 and T2 may contribute as well. • Roots Trunks Divisions Cords Terminal nerves (branches). “Robert Taylor Drinks Cold Beer”. • Terminal Branches: Axillary, Radial, Median, Musculocutaneous, and Ulnar. “ARM MU”.
Interscalene Block • Performed at the C6 level (cricoid cartilage level). • Ask patient to turn head to side. • Locate groove. • Between the anterior and middle scalene muscles. • The anterior scalene is an important landmark that should be identified. • Posterior to the posterior aspect of the SCM at the level of the cricoid. • Enter behind the External Jugular at 45 degrees caudad and posterior.
Supraclavicular Block • Needle enters 1.2cm above the middle of the clavicle. • Administer anesthetic while advancing needle towards the first rib. • Anterior-posterior direction until parasthesias are elicited.
Sciatic Nerve Block • L4-5 and S1-3 • Runs between the ischial spine and greater trochanter of the femur. • Becomes superficial at the base of the gluteus maximus. • Cutaneous innervation to posterior thigh and all of the leg below the knee minus a small medial strip. • Two approaches: Posterior and Anterior. • Usually block is combined with femoral, obturator, or lateral fem cutaneous nerve blocks. • Disadvantages: technically difficult, painful, possible hematoma, nerve damage, slight drop in BP due to blood pooling.
Posterior Approach • Lateral decub position with leg to be blocked flexed at the knee with the heel resting on the opposite knee. • Connect the posterior superior iliac spine with the greater trochanter with a drawing pen. Bisect this line perpendicularly, extending caudal. • Needle entry point: 3cm downward from the perpendicular line.
Anterior Approach • Supine position. • Line from ASIS to pubic tubercle. Mark point 2/3 of the way. • Draw parallel line from greater trochanter. • From point of first line, continue down to second line. Inject at this site until bone is hit, then direct medially.