Download
1 / 22
281 likes | 1.49k Vues
Intraoperative Cardiac Arrhythmias Cause, Recognition, and Treatment. R4 Park Sung-Wook. Occurrence: 15-85% Rare complication resulting from cardiac arrhythmia in the healthy patients Life-threatening arrhythmia during surgery Fewer than 1% of patients Almost all have cardiac disease.

E N D
Intraoperative Cardiac ArrhythmiasCause, Recognition, and Treatment R4 Park Sung-Wook
Occurrence: 15-85% • Rare complication resulting from cardiac arrhythmia in the healthy patients • Life-threatening arrhythmia during surgery • Fewer than 1% of patients • Almost all have cardiac disease
Physiology • The Action Potential
Physiology • The Action Potential • Spontaneous diastolic depolarization • Resting potential not stable in conductive tissue cell • Slow spontaneous depolarization until the threshold potential is reached Slope is controlled by ANS
Physiology • The Action Potential • Excitability: depolariztion to specific stimulus • Increased excitability • depolarization to a lesser stimuls or an exaggerated response to normal stimulus • Refractoriness • Absolute refractory period: phase 0,1,2 • Relative refractory period: late phase 3, early 4 • Susceptable to strong stimuli
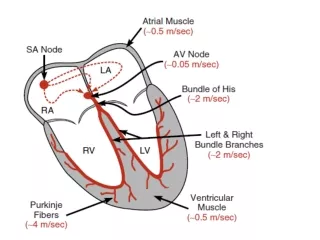
Physiology • The Conduct System Control ventricular response to increased supra ventricular rates most rapid conduction
Physiology • Electrophysiology of Arrhythmias • Disturbance of SA nodal rate • Reentry-associated arrhythmias • Alternate pathways • One-way or unidirectional block in one pathway • An area of slow conduction in the other pathway
Diagnostic Criteria • Supraventricular Arrhythmias • Rate • 150 - atrial flutter with 2:1 AV block • >200 - accessory AV pathway • Regularity • AF: irregular rhythm • Regular SVT with variable AV block may be misleading
Diagnostic Criteria • Supraventricular Arrhythmias • P waves • Presence of P wave before QRS: atrial origin • No P wave with regular tachycardia: AV node or below • QRS width • <0.12 ms: supraventricular source • Wider QRS: BBB, aberrant conduction, accessory path
Diagnostic Criteria • Supraventricular Arrhythmias • QRS axis • Severe LAD: ventricular origin • Paroxysmal SVT • Sinoatrial node reentry: normal P • Atrial tachycardias: upright but abnormal appearing P • Atrioventricular node reentry: no P or inverted • Accessory pathway: delta wave • AF: irregular narrow QRS • A-flutter: atrial rate 300 with AV block
Diagnostic Criteria • Ventricular Arrhythmias • Frequent PVCs, couplets or brief runs of VT • Healthy persons: benign • Presence of cardiac dis or LV dysfunction: dangerous • Frequent PVCs(> 6/min) after MI: increased mortality risk
Cause and Significance • Congenital • Mostly benign • Accessory pathway tachycardia: compromise hemodynamic stability • Congenital prolonged Q-T interval: predispose to vetricular arrhythmia
Cause and Significance • Acquired • Vetricular arrhythmia • IHD., aortic stenosis, dis. associated with LVH • Atrial fibrillation • IHD., related to aging, distened aorta (MS, CHF) • Acquired prolonged Q-T interval • IHD., electrolyte abnormality, drug side effect • Progress polymorphic ventricular tachycardia (torsades de pointes) • CNS dis, ICH, stroke: all types of SVT and vetricular arrhythmia
Cause and Significance • Electrolyte Imbalance • Low potassium may trigger dangerous vetricular arrhythmia • Low magnesium produce primarily SVT • Acute changes in pH • Anesthesia • Calcium antagonistic properties • Halothane: sensitize the heart to catecholamines
Treatment • Class I • Block the fast Na channel & decrease the rate of rapid depolarization • Class IA • Vagolytic action, decrease contractility, -adrenergic blockade • Quinidine, disopyramide, procainamide, diphenylhydantoin
Treatment • Class I • Class IB • Lidocaine • Used in all types of vetricular arrhythmia • Except vetricular arrhythmia d/t prolonged Q-T interval • Toxic effect: CNS activation • Class IC • Suppressor of phase 0 sodium conductance • Increased mortality risk
Treatment • Class II • ß-adrenergic receptor blockers • Effective in all tachyarrhythmias • Perioperative management of congenital prolonged Q-T interval • Toxicity related to bronchoconstriction
Treatment • Class III • Prolong reploarization • Increase action potential duration & the effective refractory period • Bretylium • Facilitation of ventricular defibrillation • Effective in bupivacaine-induced arrhythmias
Treatment • Class III • Amiodarone • Effective all arrhythmia • Long onset & half-life • Side effect: photosensitivity, abnormal skin pigmentation • Ibutilide • Effective in converting A-flutter & AF • Side effect: hypotension, prolongation of Q-T interval
Treatment • Class IV • Calcium channel antagonists • Supraventricular tachyarrhythmias: useful • Ventricular tachycardias: ineffective, severe cardiac dysfunction • Potentiate the myocardial effects of anesthetics • Contraindication: AF with WPW syndrome
Treatment • Adenosine • Effective in acutely converting reentrant nodal SVT & accessory pathway SVT • Digoxin • Perioperatively maintain rate control in A-flutter & AF • Magnesium ion • Useful in the period around CPB operations
Conclusion • Tx only associated with hemodynamic compromise and potential to progress to life-threatening arrhythmias • Must be familiar with only selective drug