UGI Bleeding
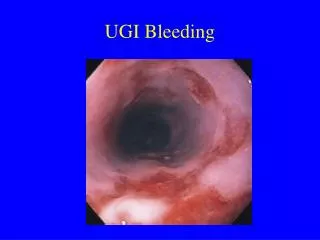
UGI Bleeding. Epidemiology of Upper GI Bleeding. Bleeding from a source above the ligament of Treitz 1 case/1,000 adults/year 50% of cases are peptic ulcer disease (25% rebleed) 40-80% of cases of bleeding cease spontaneously 10% mortality rate. Prognostic Factors. Hemodynamic instability

UGI Bleeding
E N D
Presentation Transcript
Epidemiology of Upper GI Bleeding • Bleeding from a source above the ligament of Treitz • 1 case/1,000 adults/year • 50% of cases are peptic ulcer disease (25% rebleed) • 40-80% of cases of bleeding cease spontaneously • 10% mortality rate
Prognostic Factors • Hemodynamic instability • Hematochezia from upper GI source • Increasing number of units transfused • Age > 60 years • Concurrent illness (cardiac, respiratory, renal, neoplastic, CNS) • Onset while hospitalized for other reason • Coagulopathy
Etiology of UGI Bleeding Non GI • Hemopytsis, nose bleed Esophageal • Esophagitis, ulcer, varices, malignancy, MW tear Gastric • Gastritis, ulcer, varices, malignancy, AVM Duodenal • Duodenitis, ulcer, varices, malignacy (rare), AVM, aortoenteric fistula
Etiology Incidence • PUD 50% • Esophagitis 15% • Gastritis 10% • Varices 10% • Duodenitis 5% • MW tear 3% (much more common in young) • Esophageal ulcer 3% • Carcinoma 3%
Presentation • Melena or hematochezia 70% (charting, iron pepto) • Hematemesis or coffee ground emesis 30% (charting, testing) • Syncope 14%, presyncope 40% • Heartburn 40%, epigastric pain 20% • Dysphagia 10% • Wt. loss 12%
Important History • Evidence of complications CP/SOB/presyncope • Appearance, frequency and amount of vomit/BM (elderly unreliable) • Duration of symptoms • Use of NSAID/ASA/corticosteroids • Previous history of GI bleeding • Co-morbidities = cardiac, respiratory, neoplastic, CNS
Physical Exam • ABC’s • Vitals • Orthostatic bp (scoping) • Rectal exam (what does –ve OB really mean)
Initial Management • ABC’s • Npo • Head down, raise legs • 2 IV’s • CBC • Urea/Cr (? upper vs lower bleeding, ? reliable) • G&T • LFTs • Coagulation status • ECG/cardiac enzymes • NG?
Prognostic Factors: Endoscopic Laine, Peterson, N Engl J Med1994.
Overview of Management • Initial management • Endoscopic therapy • Surgical therapy • Pharmacologic therapy
Endoscopic Therapy • Perform early (ideally within 24 h) • Indications for haemostatic therapy: • (1) +/-Adherent clot, (2) Nonbleeding visible vessel, (3) Active bleeding (oozing, spurting) (Laine, Peterson. 1994) • Heater probe, bipolar electrocoagulation or injection therapy • Decreases in rebleeding, surgery and mortality(Cook, et al. 1992, Sacks, et al. 1990)
Surgical Therapy • Endoscopic management failure • Other extenuating circumstances • Patient survival improved by optimal timing • Individualized by clinical context, endoscopic and surgical expertise
Surgical Therapy Outcomes in 92 patients with rebleeding after endoscopic therapy: endoscopic retreatment vs. surgery. Lau, et al. NEJM 1999. N/A=not applicable
Pharmacologic Therapy • Splanchnic blood pressure modifiers • vasopressin, somatostatin, octreotide • Anti-fibrinolytic agents • tranexamic acid • Acid suppressing agents • H2-receptor antagonists (H2RAs), proton pump inhibitors (PPIs)
Somatostatin/Octreotide • Effects: • Lowers splanchnic blood pressure • Decreases gastric acid secretion • Increases duodenal bicarbonate secretion • Meta-analysis: (Imperiale, Birgisson, 1997) • 14 trials (n=1,829); SOM (12 trials), OCT (2 trials) • 0.53 risk of rebleeding vs. H2RAs • RR=0.73 among investigator-blinded trials • Studies did not control for confounders, i.e., endoscopic therapy
Acid Suppressing Agents • H2-receptor antagonists (H2RAs) • Cimetidine, ranitidine, famotidine, nizatidine • Proton pump inhibitors (PPIs) • Pantoprazole, omeprazole (oral, IV) • Esomeprazole (Nexium) (oral) • Lansoprazole (oral)
Role of Acid in Hemostasis • Impairs clot formation • Impairs platelet aggregation & causes disaggregation • Accelerates clot lysis • Predominantly acid-stimulated pepsin • May impair integrity of mucus/bicarbonate barrier
Effect of PPI on Gastric pH • Increase intragastric pH • pH>6.0 for 84->99% of day • Continuous infusion (CI) superior to intermittent bolus administration • Clinical improvements in rebleeding and/or surgery with: Bolus 80 mg + CI 8 mg/h
Role of PPI For UGI Bleeding:Summary of Clinical Trials • 10 RCTs • PPI (n=1,150); controls (n= 1,142) • Minimal benefit with intermittent bolus • Clinical benefits with bolus plus continuous infusion (CI) • Decreased need for surgery and/or rebleeding • Dose: Bolus 80 mg + CI 8 mg/h x 3 d
Role of PPI For Upper GI Bleeding:Summary • H2RAs • Unlikely to provide necessary pH increases • Tolerance a problem • Minimal benefit in clinical trials • PPIs can provide profound acid suppression • pH>6.0 over 24-hours • Suggested benefits on rebleeding and/or need for surgery • Mortality benefits not yet demonstrated
Role of PPI For Upper GI Bleeding:Summary • Reasonable to consider initiating as soon as possible following presentation to hospital • Administer as bolus + continuous infusion (CI) • IV bolus 80 mg + CI 8 mg/h x 3 d • Continue therapy, probably with an oral PPI • Likely most beneficial for patients with high risk, non-actively bleeding lesions • Further trials needed to determine optimal patient group for acute IV PPI therapy
Peptic Ulcer Disease Causes: • Infectious: H.P., Herpes, CMV • Drugs: NSAIDS, corticosteroids • Neoplastic • ICU Stress Types: • DU = pain between meals • GU = pain with meals, epigastric
Peptic Ulcer Disease – Helicobacter Pylori • Most common chronic bacterial infection in man • 15% of infected go on to PUD • Dx via C13/C14 breath testing, histology, serology, urease testing (5-15% false negative) • false negative if ABO or acid suppression within the last week (except serology) • Serology $30 (not for eradication) • Breath Testing 13C non-radioactive urea metabolized to CO2 exhaled and quantified
Peptic Ulcer Disease – When to Test for H.P. • GU = test for H.P. as other causes of GU are common, especially NSAID induced ulcers, maliganancy (repeat endoscopy) • DU = if not on NSAID may treat empirically for H.P.
Helicobacter Pylori Eradication • Proven to decrease ulcer recurrence/bleeding • Tx if any history of upper GI bleeding and H.P. positive Treatment Options: • PCA= PPI + Clarithomycin 500mg bid + Amoxil 1g bid for 7 days • PCM = PPI + Clarithoromycin 500mg bid + Metronidazole 500 mg bid X 7 days (resistance)
H.P. Eradication • Antibiotics are very effective • Test for eradication only in complicated ulcer disease eg. bleeding, pyloric outlet obstruction, recurrent ulceration or persistent symptoms • Most cost effective method = breath testing • 1/12 after antibiotics are complete • 7/7 after stopping acid suppression
NSAID And Upper GI Ulceration • 2-4% annual risk of PUD related complication on NSAID (bleeding, outlet obstruction, symptomatic ulcer) • Lowest possible dose of NSAID/ASA (2-4X risk even if <325 mg ASA daily) • Prophylaxis if: • Previous PUD or GI bleed • NSAID + corticosteroids • >65 (75 in Ontario guidelines) • serious comorbidity
NSAIDS & UGI Bleeding • Classic NSAID inhibit COX-1 and COX-2 • Inhibition of COX 1 results in decreased gastric PG and hence poor protective barrier in the GI tract • COX-2 expressed predominantly in actively inflammed tissues, therefore less damage to normal GI tract • COX-2 ulcer risk approx to that of classic NSAID + PPI
COX-2 Inhibitors & UGI Ulceration • 1149 pt. with R.A. endoscopy pre and post 12 weeks therapy for GI ulceration • Compared celecoxib (2x max. dose) vs. naproxen (max. dose) vs. placebo • No difference ulceration between placebo and celecoxib vs. p<0.001 difference between celecoxib and naproxen • Near identical study with Vioxx (rofecoxib)
NSAIDS and UGI Bleeding Prophylaxis Options: • Misoprostol 200mg qid + standard NSAID • Side effects diarrhea, cramps • $38/month, 4% S/E • PPI + standard NSAID • More effective than Misoprostol • $53/month (Pantoprazole) • Cox –2 inhibitor ($40-75/month) • ? Add PPI
NSAIDS, H.P. And UGIB Prophylaxis • In high risk patients (previous PUD or ongoing dyspepsia), test and treat for H.P. prior to NSAID initiation decreases risk UGI to that of PPI or celebrex • How to test • Time consideration of breath testing • Most bleeds in first month • Previous studies show no benefit for primary prophylaxis with H.P. eradication if already on an NSAID
Esophageal Variceal Bleeding • BE SUPICIOUS, if patient is cirrhotic/heavy drinker think varices first • 30-50% mortality without early intervention • Causes of death are classically aspiration, sepsis, renal failure or encephalopathy • Treatment options: • Medical - endoscopic • Tamponade - TIPS - Surgical
Esophageal Variceal Bleeding • Medical = octreotide (72 hours) or somatostatin forget vasopressin • Endoscopic = ligation (banding), sclerotherapy
Esophageal Varices • Tamponade = Blakemore tube
Esophageal Varices TIPS = transjugular intrahepatic portosystemic shunts or Surgical Shunts = desperate measures