Key Study Results in PI Monotherapy
250 likes | 438 Vues
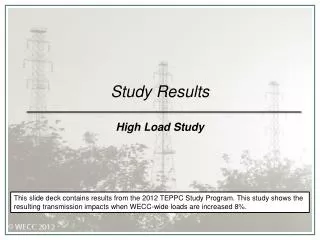
Key Study Results in PI Monotherapy. Dr. Jose R Arribas HIV UNIT. OK04 trial design. Visits : Screening , Baseline , Week 4 and 12, then every 12 weeks up to Week 96. Arribas JR. et al ., JAIDS 2009 OK04. Time to HIV-1 RNA > 50 copies/mL (ITT M = F, Reinduction = F)*. 77.6%.

Key Study Results in PI Monotherapy
E N D
Presentation Transcript
Key StudyResults in PI Monotherapy Dr. Jose R ArribasHIV UNIT
OK04 trial design Visits: Screening, Baseline, Week 4 and 12, thenevery 12 weeksup toWeek 96 Arribas JR. et al., JAIDS 2009OK04
Time to HIV-1 RNA > 50 copies/mL (ITT M = F, Reinduction = F)* 77.6% 77% % P=0.865; Log rank * Patients in the monotherapy arm who reached and maintained < 50 c/mL after resuming baseline nucleosides are considered as failures (n = 10) Arribas JR. et al., JAIDS 2009OK04
Proportion without therapeutic failure at Week 96* - 9%; upper-limit 95%CI: 1.2%. * Patients in the monotherapy arm who reached and maintained < 50 c/mL after resuming baseline nucleosides are not considered as failures (n = 10) Arribas JR. et al., JAIDS 2009OK04
Genotypic testing through Week 96 *All patients with HIV-1 RNA > 500 copies/mL analyzed (blips > 500 copies/mL included)
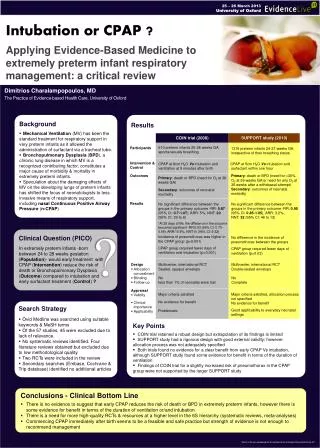
MONET - Trial Design Taking 2 NRTI + either NNRTI or boosted PI at screening (stratified) No prior use of darunavir (DRV) HIV RNA <50 copies/mL for at least 6 months, No history of virological failure DRV/r 800/100 mg OD + 2 NRTI (re-optimised at baseline) n = 129 Follow-up phase 96 weeks 256 subjects No run-in period DRV/r 800/100 mg OD n = 127 Follow-up phase 96 weeks 96 wks BL SC 30 days 4, 12, 24, 36, 48 weeks • Primary Endpoint:HIV RNA< 50 at week 48 (TLOVR). Per Protocol, Switch = Failure • 2 consecutive HIV RNA > 50 copies/mL (Roche Amplicor HIV-1 Monitor assay 1.5) • Stopping DRV/r • Starting NRTIs in the monotherapy arm • Stopping NRTIs in the triple therapy arm (switches in NRTIs were permitted at any time). J. Arribaset al, IAS Conference, Cape Town, SA, 21 July 2009, TUAB106-LB
MONET: Baseline Characteristics (ITT) Age, years (median, range) Male (%) Caucasian (%) 43 (24-72) 83% 90% 43 (25-67) 78% 92% 579 12% 6.4 (4.0) 57% 43% 48% 28% 0 15 (12%) 12 (9%) 571 14% 7.4 (4.2) 56% 44% 35% 23% 0 24 (19%) 20 (16%) Disease characteristics CD4 count (median (range), cells/uL) CD4 <350 cells/uL (%) Duration of prior ARVs, years (mean, sd) Use of PI at screening (%) Use of NNRTI at screening (%) On their first NRTI combination PI naïve Hep B Surface Antigen, positive, n (%) Hep C Antibody, positive, n (%) History of IV Drug use DRV/r +2NRTI (n=129) DRV/r (n=127) Multivariate analysis at Week 48 showed that HCV co-infection was highly predictive of response in the primary endpoint. Riegeret al. WAC July 2010, Vienna [abstr TBLBB209]
MONET: statistical methods for HIV RNA analysis Main efficacy endpoint: TLOVR, switch equals failure analysis If a patient shows a confirmed elevation in HIV RNA >50 copies/mL at two visits, this is a failure, even if the HIV RNA is then suppressed <50 copies/mL at Week 96. Stoping DRV/r in either arm, or adding NRTIs in the monotherapy arm is also a failure. Missing data is failure. Secondary endpoint: Switch included analysis This analysis only includes the HIV RNA levels at Week 96. If HIV RNA is re-suppressed at Week 96 following an earlier elevation, this is counted as success. Changes in treatment are permitted. Missing data is failure. Riegeret al. WAC July 2010, Vienna [abstr TBLBB209]
MONET: Primary Efficacy Analysis:HIV RNA <50 copies/mL at Week 48, TLOVR, S = F Per Protocol analysis (PP) Intent to Treat analysis (ITT) Primary analysis • 1.6%; lower limit 95%CI: -10.1% • 1%; lower limit 95%CI: -9.9% 100 87.8% 86.2% 85.3% 84.3% 90 80 HIV RNA <50 by Week 48 (%) 70 60 50 40 30 20 10 0 DRV/r + 2NRTI (PP) DRV/r mono (PP) DRV/r + 2NRTI (ITT) DRV/r mono (ITT) N=129 N=123 N=123 N=127 Table EFF 4-5 J. Arribas et al, AIDS 2010
MONET Week 144 analysis: HIV RNA, TLOVR, ITT Population Switch=failure Switch NRTI d/c - other d/c - AE VF HIV RNA <50 HIV RNA <50 Percentage of patients difference=-5.9%, 95% C.I.-16.9%, +5.1%).
MONET Week 144 analysis:Major IAS-USA Genotypic mutations when HIV RNA >50 copies/mL Only 1 patient per arm had any evidence of genotypic resistance
MONET Week 144 analysis:Outcome of HIV RNA elevations in DRV/r arm (21 patients)
MONET Week 144 analysis:Outcome of HIV RNA elevations in DRV/r arm (21 patients) 11
MONET Week 144 analysis:Outcome of HIV RNA elevations in DRV/r arm (21 patients) 7 3
MONET Week 144 analysis:Outcome of discontinuations in DRV/r arm (18 patients)
MONET Week 144 analysis:Outcome of discontinuations in DRV/r arm (18 patients)
Patient PL0000520Treatment arm: DRV/r Week 96 Endpoint ARV treatment started: 2002 Prior antiretrovirals taken: ABC/3TC, EFV Nadir CD4 count: 125 Hepatitis C: Antibody positive HCV RNA PCR: no data • Resistance when HIV RNA above 50 copies/mL: • Week 24: fully sensitive to NRTI, NNRTI and PI • Week 26: not amplifiable • Week 36: not amplifiable • Week 40: fully sensitive to NRTI, NNRTI and PI • DRV plasma PK levels (ng/mL): • Week 4: 4430 • Week 12: 2140 • Week 24: 1570 • Week 36: 3470 • Week 48: 2800 • Week 96: 3370 • NRTI intensification: Yes - with ABC/3TC after Week 36 Intensified onto ABC/3TC/DRV/r FAILURE by TLOVR, switch equals failure analysis NOT FAILURE by Switch included analysis HIV RNA (copies/mL) Double HIV RNA blip Time in MONET trial - weeks
MONET Week 144 analysis: HIV RNA <50 copies/mL, Switch included analysis, and observed failure (OF) Switch included analysis (PP) Observed Failure analysis (PP) TLOVR HIV RNA <50 by Week 144 (%) n=121 n=122 n=121 n=122
MONET Week 144 analysis: delta and 95% c.i.*(full multivariate analysis) HIV RNA <50 at Wk 144 DRV/r vs DRV/r +2NRTI Difference between arms Lower and upper 95% C.I. Analysis -14.6% +7.3% PP, HIV RNA <50, TLOVR, switch=failure 74.5% vs 78.2% +7.1% -15.1% Which is more clinically relevant? ITT, HIV RNA <50, TLOVR, switch=failure 71.3% vs 75.3% -7.19% +10.28% PP, HIV RNA <50 Switch included 86.72% vs 85.18% -12.9% +3.4% Observed failure TLOVR HIV RNA <50 85.5% vs 90.3% + + + DRV/r + 2NRTI better DRV/r mono better * Multivariate logistic regression, adjusting for previous PI use and factors from exploratory multivariate analysis
MONET 144 weeks: laboratory abnormalities • Differences in lipid parameters likely reflect the fact that some patients in the DRV/r + 2 NRTIs arm were taking TDF, which may have a direct lipid-lowering effect *Of the 16 patients with elevated total cholesterol in the DRV/r arm, 10 were at a single visit Arribas JR, et al. IAS 2011. Abstract MOPE216.
MONET: DRV/r MT does not increase IL-6 or hs-CRP levels • Levels of the inflammatory markers, interleukin-6 (IL-6) and C-reactive protein (CRP), are elevated in HIV-infection. • High levels of IL-6 (>3 pg/mL) and CRP (>5 mg/L) have been associated with more rapid progression to AIDS and death1 p=n.s. for both comparisons, chi-square test • There was no difference between the treatment arms in IL-6 or hs-CRP levels at the Week 144 visit • Rodger A, et al. JID 2009, 200: 973-983. Arribas JR, et al .EACS, Belgrade, Serbia, October 2011. Abstract PS 10/2.
MONOI Design Valantin MA et al. Poster 534 CROI
MONOI: Predictors of Response Marcelin AG, et al. 18th CROI; Boston, MA; February 27-March 2, 2011. Abst. 534.
A PI/r switching strategy is suggested as an option in the EACS guidelines ‘PI/r monotherapy with bid LPV/r or qd DRV/r might represent an option in patients with intolerance to NRTI or for treatment simplification. Such a strategy only applies to patients without history of failure on prior PI-based therapy and who have had viral loads <50 copies/mL in at least the past 6 months’ European AIDS Clinical Society (EACS) guidelines, 2011. Available at: http://www.europeanaidsclinicalsociety.org/images/stories/EACS-Pdf/eacsguidelines-6.pdf.