Download
1 / 27
270 likes | 511 Vues
Detailed tips for specific cranial nerve examinations, optic nerve defects, common lesions, ocular motor defects, and cerebellar exams. Includes mnemonics and lesion correlations.

E N D
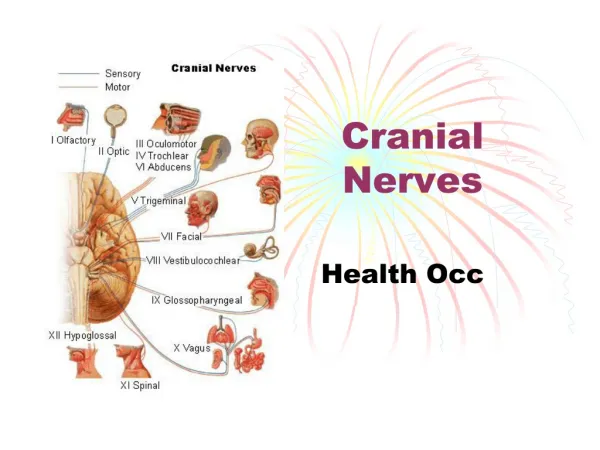
Cranial Nerves • It is very unlikely you will be asked to perform a complete examination within the time frame • Most stations will ask you to perform a SPECIFIC cranial nerve examination based around a presenting complaint • Think about common complaints, what COULD appear in OSCES (I.E nothing acute) and constellations of signs/symptoms • Nobody has been asked to do olfactory ever
EYE RELATED (CN 2, 3, 4 and 6) • An easy pneumonic is AFRO: • Acuity (Snellen’s chart) • Fields (visual fields, blind spots) • Reflexes (accommodation, direct and consensual, relative afferent pupillary defect/RAPD) • Ocular Movements (H-shape, nystagmus, ask about double vision, ptosis/lid lag)
Optic nerve defects • This could potentially be simulated by a patient. • Acuity: make sure you test each eye SEPERATELY by getting them to cover one eye each time • Fields: Blind spot isn’t usually tested (as difficult to determine whether positive result or poor technique) but visual fields are. Make sure you practice until it is smooth and make sure you’re doing one eye at a time. • Reflexes- an optic nerve defect will cause a afferent defect- pupils symmetrical, but when light is shone in affected eye, neither constrict. A RAPD may be present in MS due to damage to the optic nerve- the pupil will respond but slowly (therefore RELATIVE not DEFINITIVE). Accommodation defects are not usually tested and usually to do with myopia/hypermetropia • Unlikely to affect ocular movements unless something else is happening
Where is the lesion Common Lesions: Due to damage within the eyeball (glaucoma) PITUITARY TUMOUR Unusual, Stroke/Tumour Stroke/Tumour Stroke/Tumour Stroke/Tumour Stroke/Tumour (these seem most common, remember left hemianopia= right occipital lobe lesion
Ocular Motor Defects • Ptosis= lid lag, can be due to • 3rd nerve palsy (ipsilateral), Horner’s syndrome, Myasthenia Gravis • 3rd nerve palsy= “down and out” affected eye • 4th nerve palsy= inability to look inferiorly-medially, or diplopia which is worse on looking down • 6th nerve palsy= cant look laterally • Nystagmus has many causes, needs to be correlated with other findings
Trigeminal (5) • Sensation for the face and muscles of mastication • Just test forehead on both sides, cheek bone on both sides and angle of mandible each side • Don’t do corneal reflex its not comfortable- you can offer if you must • For muscles of mastication, ask them to clench their jaw and see if they can open it against resistance
Facial (7) • Ask them to do various facial expressions, ask about hyperacousis (“has your hearing got more sensitive”) and has their taste changed • REMEMBER: • UMN lesion, contralateral side and forehead sparing) • LMN lesion, ipsilateral side and entire side of face affected. Commonly Bell’s Palsy
Vestibulocochlear (8) • COULD come up as an ENT, asking you to do Weber’s and Renne’s testing. • Weber’s= tuning fork in middle of forehead, which side is louder: • CONDUCTS towards a CONDUCTIVE hearing loss • SNEAKS away from a SENSINEURAL hearing loss • Renne’s= confusingly, a positive Renne’s is what you’d expect to find in a healthy person (Air conduction>Bone conduction). Place fork on mastoid and then ear. If Bone>Air, then conductive hearing loss
Glossopharyngeal (9) and Vagal (10) • Unusual to test • Ask them to open mouth, say “AHH”: • Check palate symmetry for CN 9, uvula deviates AWAY from lesion for CN 10 • Ask them to swallow, difficult to check whether its one or the other • Vagal damage would cause GI and cardio problems also • Offer (don’t do) gag reflex
Accessory/ Hypoglossal (11 and 12) • Very unusual to test • Accessory is testing sternocleidomastoid muscle (turn their head against resistance) and trapezius (shrug shoulders against resistance), comment on power • Hypoglossal- ask them to stick out their tongue for you (will deviate TOWARDS the side of the lesion), comment on wasting or fasiculations
Cerebellar Exam • Main thing we’re concerned about is a cerebellar tumour or stroke. • Any positive findings could indicate cerebellar dysfunction • Useful Pneumonic is DANISH: • Dysdiadochokinesia • Ataxia (gait and posture) • Nystagmus • Intention tremor • Slurred, staccato speech • Hypotonia/Heel-shin test
How I would do it: • Start in the hands • Then do the “arms” • Work up towards the face • Finally do gait and posture
Hands • Dysdiadochokinesia= watch a video if you’ve not seen this. Basically just asking them to turn their hand over and over in their other hand, as fast and as smooth as possible. • Intention Tremor= ask them to touch their nose and then FULLY OUTSTRETCH their hand to touch your finger. Get them to repeat whilst you slowly move your finger about. Intention tremor occurs at the END of the movement whilst an ACTION tremor occurs all the way through.
ARM • OFFER TO (might save some time): • Assess tone= MAY be reduced in cerebellar dysfunction but often normal • Assess reflexes= MAY be pendular(less brisk and slower to rise and fall) but unlikely to be changed • Test pronator drift • Test Rebound Phenomenon
Rebound Phenomenon • Whilst the patient’s arms are still outstretched and their eyes are closed: • 1. Ask the patient to keep their arms in that position as you press down on their arm. • 2. Release your hand. • 3. When resistance is suddenly removed, a healthy patient’s limb normally moves a short distance in the desired direction and then rebounds (jerks back in the opposite direction) • An exaggerated response is due to spasticity, a diminished response is due to cerebellar dysfunction
Face • Nystagmus= Test using the H-shape: • As a rule, nystagmus has a slow and a fast phase, and the fast phase will be in the direct of the cerebellar lesion- but this is advanced stuff • Hold up hand about 30cm to the side of the face, ask them to look between your face and your hand rapidly- STACCADES is where the eye movement is jerky and overshoots • Ask them to say “British constitution” and “baby hippopotamus” to test for Slurred Speech
Gait • N.B can ask them to do a heel-to-shin test whilst still lying down • Check for walking aids around the bed • Assess gait generally, then ask them to do heel-to-toe walking, which can be more sensitive. • Will often walk like a drunk person, unsteady wide based gait • Often veer to side of lesion • Perform Rhomburg’s Test: ask them to stand still with their eyes closed, be ready to catch them: • Swaying a bit is normal, shouldn’t fall over • If they fall quickly it indicates a sensory ataxia and can be useful to distinguish between cerebellar and sensory ataxia
Parkinson’s Examination • Broadly looking for 4 things: • Bradykinesia • Rigidity • Gait/Postural Instability • Tremor • Usually station will say “examine this patient with a tremor” or “assess this patient’s gait and proceed” • Best to be on the lookout, usually fairly obvious
Gait • If the patient is not sat down, I will first ask them to walk across the room, noting: • Stooped posture • Hesitancy starting and turning • Difficulty stopping (festination) • Small, shuffling steps • Lack of arm swing (bradykinesia)
Tremor • A resting tremor in Parkinson’s should be unilateral (unless highly progressed), usually involves hand but may involve leg, described as pill-rolling. • Will reduce if patient is actively noting it, so ask them to close eyes and count back from 10 to accentuate it (unless its clearly noticeable without this). • Also ask them to hold arms out at length with eyes closed to check for postural tremor (although a resting tremor may return after a period of stability in this position) and do finger-to-nose testing for intention tremor
Bradykinesia • Ask them to clap their thumb and index finger together on both hands as fast and as firmly as possible (demonstrate what you mean) • In Parkinson’s they will struggle with this and it will become weaker and slower • You can do the same with asking them to tap their feet as if to a rhythm- will lose time/slow down • Usually do it for 15-20 seconds
Rigidity • Parkinson’s gives somebody a hypertonic, Velocity-Independenttone (will be constantly stiff regardless of speed of passive movement) • Often called Lead-Pipe rigidity. • Cog-wheel rigidity is due to a tremor superimposed on the increased tone
Other Tests • Also in Parkinson's • Micrographia- ask them to write something • Hypomimia- reduced facial expressions • Slow, monotone speech • Difficulty doing up buttons (useful assessment of functional ability but don’t labour it) • Parkinsonism PLUS: • Inability to look up: Progressive Supranuclear Palsy • Labile Blood Pressure/Nystagmus: Multi-system Atrophy
To Conclude: • A full history • Medication check (some drugs cause Parkinsonian symptoms) • Cerebellar exam • Postural Blood pressure (MSA) • Mini mental state exam (Lewy Body Dementia/Depression [present in up to 40% of Parkinson patients) • Doesn’t usually require specialised imaging