Download
1 / 33
350 likes | 842 Vues
Ischaemic Heart Disease . Geraldine Murphy FY1 in COTE NMGH. Classification of IHD Anatomy Pathology Epidemiology and risk factors Primary prevention Acute management . Investigations Reperfusion Secondary prevention Surgery Complications post MI ECG quiz Questions . Summary .

E N D
Ischaemic Heart Disease Geraldine Murphy FY1 in COTE NMGH
Classification of IHD Anatomy Pathology Epidemiology and risk factors Primary prevention Acute management Investigations Reperfusion Secondary prevention Surgery Complications post MI ECG quiz Questions Summary
Ischaemic Heart Disease • Stable angina • Acute coronary syndrome • Unstable angina • Myocardial infarction • NSTEMI • STEMI
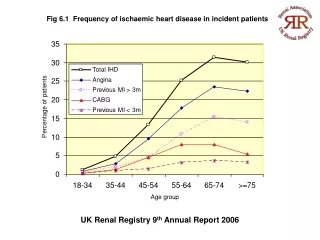
Facts and figures • MI occurs every 2 mins in UK • Account for 100,000 deaths annually • Cardiovascular death accounts for 40% all deaths under the age 75 yrs • Major cause of cardiac arrest • Survival to discharge of all rhythm cardiac arrests is 10.7%
Mechanisms of ischaemia • Ischaemia – disturbance in myocardial oxygen supply and demand • Impaired coronary artery blood flow • Atherosclerosis • Coronary artery spasm • Dissection • Tachycardia – shortened diastole • Impaired oxygen delivery • Hypoxia • Anaemia • Increased cardiac work
Pathology of atherosclerosis • Lipid laden macrophages form fatty streak • This allows lipids to deposit in the arterial wall • Smooth muscle cells, cholesterol and lymphocytes also join the plaque • Eventually a fibrous cap forms around the whole structure causing a narrowing • Causes ischaemia by three mechanisms • Platelet aggregation can form clots – emboli • Plaque rupture • Progressive stenosis
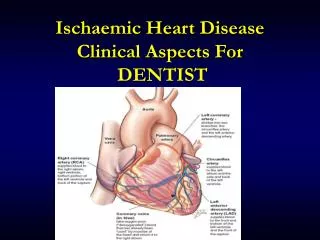
Anatomy • Aorta • Right Coronary Artery • Left Anterior Descending Artery • Circumflex Coronary Artery • Left main stem
Circumflex artery obstruction • Lateral infarction • ECG changes leads I, AVL and V4-V6 • 20% cases • Left anterior descending obstruction • Anterior infarction • ECG changes V1-V4 • 50% cases – most likely to cause left ventricular dysfunction
Right coronary artery obstruction • Inferior infarction • ECG changes in II, III & AVF • 30% cases - often causes bradyarrythmias • Posterior myocardial infarction • Usually right coronary artery but may be circumflex • ST depression in anterior leads • Dominant R wave is actually a Q wave
Fixed Age Male sex Menopause Family history Diabetes Rheumatoid arthritis Modifiable Smoking Hypertension Hyperlipidaemia Obesity Alcohol Sedentary lifestyle Risk Factors
Stable angina • Myocardial ischaemia without muscle necrosis • Caused by • Fixed stenosis • Coronary artery spasm • Other disease – hypoxia, valvular disease • History • Exercise related, pressing precordial chest pain, can radiate to jaw and left arm, often relieved by nitrates. • Can also manifest as breathlessness
Stable angina • Investigations • ECG • Often normal or non specific changes such as T wave inversion, can show ST depression reflecting ischaemia • Exercise ECG • ECG changes related to exertion – particularly ST depression, dysrhythmias, hypotension
Stable Angina – Management • Lifestyle modification • Stop smoking • Good diabetic control • Cut down alcohol • Lose weight – reduces myocardial work • Symptom control • Nitrates – dilate coronary arteries • Rest
Stable angina – Management • Drug therapy • Antihypertensives • Statins – help prevent plaque rupture, ↓ LDL • Aspirin – antiplatelet • Beta blockers • Antagonists of adrenaline & noradrenaline • Reduced contractility and heart rate • Calcium antagonist • Vasodilation (especially dihydropyidines) • Prolongation of action potential, antidysrrythmic
Stable angina – Management • Coronary revascularisation • Angina post myocardial infarction • Unstable angina • Severe IHD • Stable angina uncontrolled by medication
Acute Coronary Syndrome • History Site – Left sided/central chest pain Onset – sudden, can occur at rest Character – dull, burning, sense of doom Radiation – jaw, left arm, neck Associated factors – sweating, nausea, vomiting, breathlessness, palpitations Timing – >20mins, unrelieved by rest Exacerbating/ relieving factors Severity – Like normal angina but much worse Risk factors
Cardiac sounding chest pain ECG – non specific changes (T wave inversion, ST depression, Q waves, AF) Normal ECG ECG – ST elevation STEMI 12 hour troponin I Negative Trop I Positive Trop I Reperfusion Unstable angina NSTEMI Thrombolysis PCI Medical management Medical Management
Immediate Management • Airway • Breathing – oxygen, RR, sats, creps • Circulation – BP, HR, cannula, bloods, monitoring if unstable, CRT • Disability – GCS, BM • Exposure – Other causes for chest pain, abdomen, calves
Immediate Management • MONA • Morphine – analgesia and reduced preload • Metoclopramide (avoid cyclizine) • Oxygen • Nitrates – vasodilator • Aspirin 300mg, Clopidogrel 300mg
Investigations • ECG - initially hyperacute T waves, then ST elevation, then T wave inversion then Q waves • Chest x-ray • Bloods – FBC, U&Es, LFTs, Glucose, Cardiac enzymes • ? Echo • CCU monitored bed
Indications for reperfusion • ST elevation >0.2 in 2 adjacent chest leads • ST elevation >0.1 in 2 adjacent limb leads • Dominant R waves and ST depression in V1-V3 (posterior infarct) • New LBBB
Reperfusion Therapy • Percutaneous Coronary Intervention • Used for STEMI as these suggest full thickness infarction • Should be done in <90mins • Method: Occluded vessel identified, guidewire passed, balloon inserted, stent inserted • Advantages • Culprit artery re-opened to normal calibre • Lower risk of major bleeding
Reperfusion Therapy • Thrombolysis • Advantages – easy to perform, can be done quickly • Disadvantages • Inability to achieve reperfusion in all cases • Risk of inducing bleeding • Cannot detect success of reperfusion • Contraindications • Recent CVA or previous haemorrhagic stroke • Recent surgery • Active bleeding
Secondary prevention • Low Molecular Weight Heparin 1mg/kg OD • Aspirin • Clopidogrel • Beta blocker – usually Bisoprolol • ACE inhibitor – usually Ramipril • Glycoprotein IIb/IIIa inhibitor • Statin • Omacor • Cardiac rehabilitation
CABG • Usually reserved for severe triple vessel disease not amenable to PCI • Two forms • Vein grafts – leg saphenous veins, quick to apply, annual failure 8% • Arterial grafts – more technically difficult, better long term survival, uses internal mammary artery • 1% mortality if elective • Prior to surgery – optimise diabetes, do pulmonary function tests and vein mapping
Complications • • Sudden death on PRAED Street • • P- pump failure • • R- rupture of papillary muscle or septum • • A- aneurysm and arrhythmias • • E- embolism • • D- Dressler’s syndrome
Immediate - Dysrhythmias • Ventricular tachycardia/fibrillation– usually respond well to resuscitation • Sinus tachycardia – heart failure or anxiety • Sinus bradycardia – early change particularly with inferior infarcts – can treat with atropine • Atrial fibrillation – poor prognosis as indicates myocardial damage • Complete heart block • Inferior MI usually resolves alone • Anterior MI – bad prognosis, may need pacemaker
Heart failure • Left ventricular dysfunction can lead to hypotension, pulmonary oedema and renal impairment • Treatment – diuretics, nitrates, ACE inhibitor, later a beta blocker • Cardiogenic shock – very poor prognosis
Other complications • Pericarditis – 48hrs after full thickness MI, widespread ST elevation • Septal rupture – acute haemodynamic deterioration, pansystolic murmur, treatment is surgery (2-5 days) • Ruptured papillary muscle – causes mitral prolapse (hours – days) • Left ventricular aneurysm – persistent ST elevation • Mural thrombus – secondary to poor LV contraction • Dressler’s syndrome – self limiting autoimmune pericarditis 2-3 weeks post MI
Potential OSCE stations Record an ECG and then interpret results Interpret chest X-ray with pulmonary oedema Chest pain history Cardiovascular examination Write up drug chart for acute ACS and secondary prevention ILS Counselling post MI re risk factors Emergency history and treatment station
Post MI counselling • Explain medications and their use • 2 months off work and avoid heavy labour • Avoid sex for one month • Build up exercise gently • Stop smoking • Reduce alcohol • Avoid driving for 4-6 weeks • Avoid flying for 2 months