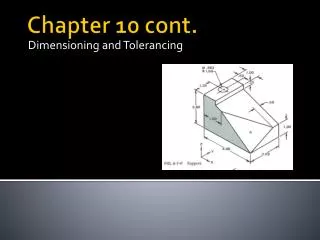
Understanding Down Syndrome: Causes, Development, and Health Concerns
This chapter explores Down syndrome, the most common autosomal trisomy caused by an extra chromosome 21. It discusses key concepts: nondisjunction during gametogenesis, the impact of maternal age, and how karyotyping can diagnose the condition. We delve into developmental aspects of children with Down syndrome, their physical features, and the genetic variations, such as translocation and mosaicism. The text highlights potential health concerns, including hearing deficits, heart disease, and obesity, culminating in an overview of current research on genetic treatment possibilities.

Understanding Down Syndrome: Causes, Development, and Health Concerns
E N D
Presentation Transcript
Chapter 15 cont. Biology
A. Karotypes shows chromosomes paired according to size, shape, and appearance in metaphase. can be used to diagnose chromosomal abnormalities.
B. Nondisjunction Causes Abnormalities • failure of one or more chromosomes to separate. • Study of spontaneous abortions suggests many trisomies and nearly all monosomies are fatal.
C. Down Syndrome • 1. Most common autosomal trisomy, involves chromosome 21. • 2. Most often, Down syndrome is due to nondisjunction during gametogenesis.
C. Down Syndrome • a. In 23% of cases, the sperm had the extra chromosome 21. • b. In 5% of cases, there is translocation where chromosome 21 is attached to chromosome 14.
C. Down Syndrome • 3. Chances of a woman having a Down syndrome child increase with age. • 4. Chorionic villi sampling or amniocentesis and karyotyping detects a Down syndrome child.
C. Down Syndrome • 5. Down syndrome child has tendency for leukemia, cataracts, faster aging, and mental retardation. • 6. Gart gene, located on bottom third of chromosome 21, leads to high level of purines; is associated with mental retardation; future research may lead to suppression of this gene.
How do children with Down syndrome develop? • Children with Down syndrome are usually smaller • physical and mental developments are slower • mild to moderate range of mental retardation, however, some children are not mentally retarded at all • motor development is slow and instead of walking by 12 to 14 months as other children do, children with Down syndrome usually learn to walk between 15 to 36 months. • Language development is also markedly delayed.
What are the physical features of a child with Down syndrome? • flattening of the back of the head • slanting of the eyelids • small skin folds at the inner corner of the eyes • depressed nasal bridge • slightly smaller ears, small mouth • decreased muscle tone, loose ligaments, and small hands and feet • About fifty percent of all children have one line across the palm, and there is often a gap between the first and second toes
How may chromosome subtypes are observed in Down syndrome? • 1. 95 percent have an extra 21 chromosome. Instead of the normal number of 46 chromosomes in each cell, the individual with Down syndrome has 47 chromosomes. This condition is called trisomy 21. • 2. 3 - 4 percent of the individuals with Down syndrome have a translocation since the extra 21 chromosome is attached, usually on chromosome 14, 21 or 22. I • 3.Another chromosome problem, called mosaicism, is noted in about 1 percent of individuals with Down syndrome. In this case, some cells have 47 chromosomes and others have 46 chromosomes. Mosaicism is thought to be the result of an error in cell division soon after conception.
Can Down syndrome be medically treated? • Although many medications and various therapies have been touted as treatment for people with Down syndrome, there is no effective medical treatment available at the present time. However, recent advances in molecular biology make it feasible now to examine the genetic basis for Down syndrome. Once we identify the genes on chromosome 21 ( many already have been discovered) and once we find the mechanism of how these genes interfere with normal developmental sequences, and if one could counteract these specific actions, a rational approach to medical therapy could emerge.
What health concerns are often observed in people with Down syndrome? • 1.Sixty to 80 percent of children with Down syndrome have hearing deficits. • 2.Forty to 45 percent of children with Down syndrome have congenital heart disease. • 3.Intestinal abnormalities also occur at a higher frequency in children with Down syndrome. For example, a blockage of the esophagus, duodenum, and at the anus are not uncommon in infants with Down syndrome. • 4. 3 percent of infants with Down syndrome have cataracts. Other eye problems such as cross-eye (strabismus), near-sightedness, far-sightedness. • 5. Obesity is often noted during adolescence and early adulthood. • 6.Skeletal problems have also been noted at a higher frequency in children with Down syndrome, including kneecap subluxation (incomplete or partial dislocation), hip dislocation, and atlantoaxial instability. • 7.Other important medical aspects in Down syndrome, including immunologic concerns, leukemia, Alzheimer disease, seizure disorders, sleep apnea and skin disorders, may require the attention of specialists in their respective fields.
What is the cause of Down syndrome? • Although many theories have been developed, it is not known what actually causes Down syndrome. Some professionals believe that hormonal abnormalities, X-rays, viral infections, immunologic problems, or genetic predisposition may be the cause of the improper cell division resulting in Down syndrome. • It has been known for some time that the risk of having a child with Down syndrome increases with advancing age of the mother; i.e., the older the mother, the greater the possibility that she may have a child with Down syndrome. However, most babies with Down syndrome (more than 85 percent) are born to mothers younger than 35 years. Some investigators reported that older fathers may also be at an increased risk of having a child with Down syndrome. • It is well known that the extra chromosome in trisomy 21 could either originate in the mother or the father. Most often, however, the extra chromosome is coming from the mother.
D. X and Y Numbers Also Change • 1. XYY males withJacob syndrome have two Y chromosomes instead of one. • a. Usually taller than average; suffer from persistent acne; tend to have lower intelligence. • b. Earlier claims that XYY individuals were likely to be aggressive are not correct.
D. X and Y Numbers Also Change • 2. Turner(XO)syndromefemales have only one sex chromosome, an X. • a. Turner females are short, have a broad chest and webbed neck. • b. Ovaries of Turner females never become functional; therefore, do not undergo puberty.
D. X and Y Numbers Also Change • 3. Klinefelter syndromemaleshave one Y chromosome and two or more X chromosomes. • a. Affected individuals are sterile males; testes are underdeveloped. • b. Individuals have large hands and feet and long arms and legs.
D. X and Y Numbers Also Change • 4. Triplo-X females have three or more X chromosomes. • a. There is no increased femininity; most lack any physical abnormalities. • b. May experience menstrual irregularities, including early onset of menopause.
E. Fragile X Syndrome • 1. X chromosome is nearly broken; most often found in males. • 2. As children: hyperactive or autistic; delayed speech.
E. Fragile X Syndrome • 3. As adults: large testes, unusually protruding ears. • 4. Occurs in females, but symptoms are less severe. • 5. Passes from symptomless male carrier to grandson.
D. Pedigree Charts • 1. Pedigree charts show pattern of inheritance within a family.
D. Pedigree Charts • 3. A carrier is a heterozygous individual who has no apparent abnormality but can pass on an allele for a recessively inherited genetic disorder.
D. Pedigree Charts • 4. Autosomal dominant and autosomal recessive alleles have different patterns of inheritance.
1. Neurofibromatosis • a. This is an autosomal dominant disorder that affects one in 3,000 people. • b. Affected individuals have tan skin spots at birth, which develop into benign tumors.
1. Neurofibromatosis • c. Neurofibromas are comprised of nerve cells or other cell types. • d. Most case symptoms are mild, patients live a normal life; sometimes symptoms are severe:
1. Neurofibromatosis • 1) skeletal deformities, including a large head; • 2) eye and ear tumors that can lead to blindness and hearing loss; and • 3) learning disabilities and hyperactivity.
1. Neurofibromatosis • e. Gene that codes for neurofibromatosis is huge; includes three smaller nested genes. • 1) It is a tumor-suppressor gene active in controlling cell division. • 2) When it mutates, a benign tumor results.
2. Huntington Disease • a. This is also an autosomal dominant disorder that affects one in 20,000 people. • b. It leads to progressive degeneration of brain cells, which in turn causes severe muscle spasm, personality disorders, and death in 10-15 years from onset.
2. Huntington Disease • e. Gene contains many repeats of base triplet CAG; normal persons have 11- 34 copies; affected persons have 42- 120 or more copies. • f. Severity and time of onset of associated disorders depend on number of triplet repeats.
1. Tay-Sachs Disease • a. Usually occurs among Jewish people in the U.S. of central and eastern European descent.
1. Tay-Sachs Disease • b. Symptoms are not initially apparent; infant's development begins to slow at 4-8 months, neurological and psychomotor difficulties become apparent, child gradually becomes blind and helpless, develops seizures, eventually becomes paralyzed, dies by age of three or four.
1. Tay-Sachs Disease • c. Results from lack of enzyme hexosaminidase A (Hex A) and subsequent storage of its substrate, glycosphingolipid, in lysosomes.
1. Tay-Sachs Disease • d. Primary sites of storage are cells of the brain; accounts for progressive deterioration. • e. No treatment or cure; prenatal diagnosis is by amniocentesis and chorionic villi sampling.