Download
1 / 24
250 likes | 517 Vues
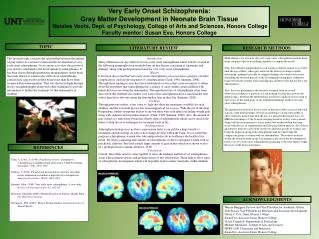
Early Onset Childhood Schizophrenia. The Basics and their relation to January “Jani” Schofield No part of this presentation may be replicated without the explicit permission of Susan and Michael Schofield and Amelia Davis. MD. PhD. What is Schizophrenia?.

E N D
Early Onset Childhood Schizophrenia The Basics and their relation to January “Jani” Schofield No part of this presentation may be replicated without the explicit permission of Susan and Michael Schofield and Amelia Davis. MD. PhD
What is Schizophrenia? • Schizophrenia is a Neuropsychiatric Disorder characterized by severe impairments in interpreting reality. Schizophrenia has both positive and negative symptoms • A) Positive Symptoms are symptoms that are ADDED to a person…such as hearing voices, seeing visions, feeling things crawling a person’s skin. One can also smell things that are not there (this is not always the most common).
What is Schizophrenia Cont. • 1) Hallucinations: Hallucinations deal with the 5 senses. They involve hearing voices, seeing people or objects or animals, odd skin sensations, and occasionally smell. • 2)Delusions: are misinterpretations of thought that cannot be shaken in the face of realistic and actual evidence. They include paranoid feelings • B) Negative Symptoms are symptoms that are taken away from a person. These symptoms include the inability to care for one’s own personal grooming ( such as age appropriate developmental skills as getting dressed). • Cognitive Dysfunction: Children with schizophrenia can have memory impairments and lower IQ scores.
The Causes • The Causes of Schizophrenia are not clear. They involve a genetic influence, a societal- behavioral influence, Prenatal brain damage, maternal depression and paternal age. • A) It is important to remember that NO-ONE is at fault for Schizophrenia, least of all the patient.
Treatments • There is NO cure for Schizophrenia but there are many treatments that help alleviate the symptoms and allow patients to lead productive lives. • Anti-psychotics: Are medicines that interact with the Dopamine Receptors in the brain thereby alleviating the amount of Dopamine the receptors use.
Treaments Cont. • Anti-depressants (SSRI’s, SSNRI) work on the Serotonin and Nor-epinephrine receptors in the brain thereby altering the amount of Serotonin and Nor-epinephrine used in signal processing. These are often used to alleviate the depressive symptoms seen in Schizophrenics • Mood Stabilizers: Are medicines that prevent the mood from DROPPING low and SOARING high. The meds are have dual purpose and are often anti-seizure meds such as Tegretol.
Treatments Cont. • Behavioral Cognitive Therapy: This is a special type of therapy that assists the patient in changing his way of thinking or monitoring his thoughts so that negative behaviors, and thereby negative consequences, can be alleviated. • Play Therapy: Is a special type of kid centered therapy that allows a child to “play” and come to terms in dealing with his or her illness.
The Difference Between Psychiatry and Psychology • Psychology: is an academic and applied discipline which involves the scientific study of animal mental function and behaviors without the use of medicine (though often augmented by a psychiatrist. • Psychiatry: is the medical specialty devoted to the study and treatment of mental disorders with the use of medicine. • BOTH are very important in the long term treatment of Schizophrenia.
Early Infancy Symptoms • Jani was probably born with Childhood Schizophrenia • Her early symptoms exhibited as lack of lengthy sleep usually seen in young infants • An apparent tracking of “unseen” objects at infancy • A constant need for ongoing and long lasting stimulation
Brief Timeline • Lack of co-play at around age four • Talking in Strange Voices at age 5 (especially immediately after the birth of her brother • -Aug 2005: Hallucination "Low"shows up • 2006: Begins psychotic screaming and lashing out at her friends (out of character for her) • -Fall of 2007: IQ tested at above 130 (146) • -Fall of 2007: Jani told her mother that she lived in two different worlds. • -2007: Jani begins violent outburst • -2007: Jani stopped showing emotions except for anger • -2007: Referral to a psychiatrist • Dec 2008- Jani in severe protracted psychosis • Dec 2008-Jani referred for AB3632, evaluating psychologist recommended Residential due to violence against Bodhi and no signs of prolonged stabilization • Jan 16, 2009 Extreme psychosis, Parent's refused to take her home, Ambulance called. Jani admitted to UCLA
Some More Important Dates • March 19: Doctor's at UCLA are leaning towards a diagnosis of childhood schizophrenia; Jani is given a 50/50 chance of being a functional adult. Jani is violent towards Bodhi investigating her belongings. Jani played with a hallucination called 24 hours. • April 19: Jani was assigned at 1:1 on the ward. She woke up at 4:30am, left her room and was violent towards staff. PRN Benadryl given at 6:00am at 10:30am another PRN Benadryl was given. Jani attempted to fight the affects and had another incident. Jani was placed in her room for a time-out and bit the furniture so hard it drew blood. Jani did not recognize her father. Jani stated it was 200 degrees in Calalini that day
April 19: Jani was assigned at 1:1 on the ward. She woke up at 4:30am, left her room and was violent towards staff. PRN Benadryl given at 6:00am at 10:30am another PRN Benadryl was given. Jani attempted to fight the affects and had another incident. Jani was placed in her room for a time-out and bit the furniture so hard it drew blood. Jani did not recognize her father. Jani stated it was 200 degrees in Calalini that day
Her Hallucinatory Friends • Low, 400 the Rat (neg-command) , 24 hours, 100 degrees, Midnight (1), Wednesday the Cat (neg-command), 6 Cat's named after the rest of the week. July 4-cat
Her Medicine • Thorazine (an older anti-psychotic that primarily works on the D2 dopamine receptor • Clozaril: The best but most dangerous anti-psychotic. Clozaril works primarily on the D4 dopamine receptor. • 1) Clozaril has 5 black box warnings!! • 2)www.clozaril.com • Lithium: Lithium is a mood stabilizer and helps with impulse control.
Her Routine • Jani is constantly on the go! Her parent’s have found that constant stimulation is the best way to keep Jani out of a psychosis • Her parents have separated her brother and her into two different apartments in order to alleviate her stress (and his). • Jani is constantly worried about Bodhi “messing with her stuff” (Paranoid Delusions) • In Jani’s apartment her parent’s try and follow the psychiatric wards routine with Recreational Therapy, Occupational therapy all set at prescribed times
How you can help • Keep in mind this is a learning experience. • 1) so read, read, read on the topic!!! • Keep in mind that Jani is intellectually very smart. • Keep in mind that Jani’s emotional maturity is that of a 2-3 year old child
Violence • NO ONE likes to be hit and Jani does often lash out and hit those around her. • 1) It is especially hard to take when you are volunteering your time and energy to help someone. • Keep in mind that Jani has little to no control over herself when she is a psychosis and she cannot express her emotions well even when she is not in a psychosis • It is important to remember that your job is to cut hitting opportunities off at the pass.
If you find yourself hit by Jani, do your best to ignore it, if possible, while redirecting her into a more appropriate activity. • Give her the appropriate language to express herself: “You are angry”, “You are frustrated”, “You wish mom or dad would hurry up, slow down, etc”.
Plan of Action • Go into your internship time with a “plan of action”. • 1) Have preset and organized things or ideas for your time together BEFORE you entire the apartment or car, etc • 2) As a rule…preplan 2 days of activities for a 4-5 hour session. • 3) When you enter the apartment, ask about her day, how she is feeling, has she already had her meds..this gives you a “heads up”.
4) If Jani has a “meltdown” it is important to immediately check for safety.. • A) is the furniture moved away from her? • B) are there sharp objects in the way? • C) try a bit of “music grounding” pick a simple song and sing it softly to her. • D) Do not try and “stop” the meltdown if it continues for more then a few minutes…it is best to let work itself out..with you being the “safety monitor”. • E) Attempt to keep yourself towards the back of her body (avoids getting hit, smacked, etc.) but with some physical contact. • F) If it does not simmer down…let Michael and/or Susan handle it and you can help by following directions during the moment.
Coping Mechanisms • If you are shaken up by the outburst… • 1) Immediately take a deep breathe and exhale rapidly. • 2) After Jani is safely with her parents…give yourself a little time to regroup. • 3) Talk about what you saw with your professor, and/or with other interns as it can be very scary to watch!
What NOT to do • Attempt to physically restrain her (that is Michael and Susan’s job) • Show up late to your preplanned session • 1) Jani develops relationships with you guys! • Not have some plan of action in your head before your time. • Not read and learn everything you can about Schizophrenia. • Give up!