Download
1 / 69
790 likes | 1.29k Vues
24 Fluid, Electrolyte, and Acid-Base Balance. Section 1: Fluid and Electrolyte Balance. Learning Outcomes 24.1 Explain what is meant by fluid balance, and discuss its importance for homeostasis. 24.2 Explain what is meant by mineral balance, and discuss its importance for homeostasis.

E N D
24 Fluid, Electrolyte, and Acid-Base Balance
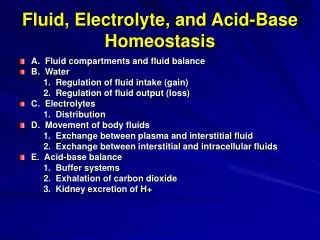
Section 1: Fluid and Electrolyte Balance Learning Outcomes 24.1 Explain what is meant by fluid balance, and discuss its importance for homeostasis. 24.2 Explain what is meant by mineral balance, and discuss its importance for homeostasis. 24.3 Summarize the relationship between sodium and water in maintaining fluid and electrolyte balance. 24.4CLINICAL MODULE Explain factors that control potassium balance, and discuss hypokalemia and hyperkalemia.
Section 1: Fluid and Electrolyte Balance Fluids constitute ~50%–60% of total body composition Minerals (inorganic substances) are dissolved within and form ions called electrolytes Fluid compartments Intracellular fluid (ICF) Water content varies most here due to variation in: Tissue types (muscle vs. fat) Distinct from ECF due to plasma membrane transport Extracellular fluid (ECF) Interstitial fluid volume varies Volume of blood (women < men)
Figure 24 Section 1 1 Total body composition of adult males WATER 60% Total body composition of adult males and females ICF ECF Interstitialfluid 21.5% Intracellularfluid 33% Plasma 4.5% Solids 40%(organic and inorganic materials) Other body fluids (≤1%) SOLIDS 40% Adult males Total body composition of adult females WATER 50% ECF ICF Interstitialfluid 18% Intracellularfluid 27% Plasma 4.5% Other body fluids (≤1%) Solids 50%(organic and inorganic materials) SOLIDS 50% Adult females
Figure 24 Section 1 2 The solid components of a 70-kg (154-pound)individual with a minimum of body fat SOLID COMPONENTS (31.5 kg; 69.3 lbs) Kg Miscellaneous Lipids Carbohydrates Proteins Minerals
Module 24.1: Fluid balance Fluid balance Water content stable over time Gains Primarily absorption along digestive tract As nutrients and ions are absorbed, osmotic gradient created causing passive absorption of water Losses Mainly through urination (over 50%) but other routes as well Digestive secretions are reabsorbed similarly to ingested fluids
Figure 24.1 2 Dietary Input Digestive Secretions Food and drink 2200 mL Saliva 1500 mL The digestive tract sites of water gainthrough ingestion or secretion, or waterreabsorption, and of water loss Gastric secretions 1500 mL 5200 mL Liver (bile) 1000 mLPancreas (pancreaticjuice) 1000 mL Water Reabsorption Intestinal secretions 2000 mL 9200 mL Small intestinereabsorbs 8000 mL 1200 mL Colonic mucous secretions200 mL Colon reabsorbs 1250 mL 1400mL 150 mL lostin feces
Module 24.1: Fluid balance ICF and ECF compartments balance Very different composition Are at osmotic equilibrium Loss of water from ECF is replaced by water in ICF = Fluid shift Occurs in minutes to hours and restores osmotic equilibrium Dehydration Results in long-term transfer that cannot replace ECF water loss Homeostatic mechanisms to increase ECF fluid volume will be employed
Figure 24.1 3 Water absorbed acrossdigestive epithelium(2000 mL) The major factors that affect ECF volume Water vapor lost in respiration andevaporation frommoist surfaces(1150 mL) Metabolicwater(300 mL) Water lost in feces (150 mL) ECF ICF Water secretedby sweat glands(variable) Plasma membranes Water lost in urine(1000 mL)
Figure 24.1 4 Changes to the ICF and ECF when water losses outpace water gains Intracellularfluid (ICF) Extracellularfluid (ECF) The ECF and ICF are inbalance, with the twosolutions isotonic. Water loss from ECFreduces volume andmakes this solutionhypertonic with respectto the ICF. ECF water loss An osmotic water shiftfrom the ICF into theECF restores osmoticequilibrium butreduces the ICF volume. IncreasedECF volume Decreased ICF volume
Module 24.1 Review a. Identify routes of fluid loss from the body. b. Describe a fluid shift. c. Explain dehydration and its effect on the osmotic concentration of plasma.
Module 24.2: Mineral balance Mineral balance Equilibrium between ion absorption and excretion Major ion absorption through intestine and colon Major ion excretion by kidneys Sweat glands excrete ions and water variably Ion reserves mainly in skeleton
Figure 24.2 1 Mineral balance, the balance between ion absorption (in the digestive tract) and ion excretion (primarily at the kidneys) Ion Excretion Ion Absorption Ion reserves (primarilyin the skeleton) Sweat glandsecretions(secondarysite of ion loss) Ion absorption occurs across theepithelial lining of the small intestineand colon. Ion pool in body fluids Kidneys(primary siteof ion loss) ICF ECF
Module 24.2 Review a. Define mineral balance. b. Identify the significance of two important body minerals: sodium and calcium. c. Identify the ions absorbed by active transport.
Module 24.3: Water and sodium balance Sodium balance (when sodium gains equal losses) Relatively small changes in Na+ are accommodated by changes in ECF volume Homeostatic responses involve two parts ADH control of water loss/retention by kidneys and thirst Fluid exchange between ECF and ICF
Figure 24.3 1 The mechanisms that regulate sodium balancewhen sodium concentration in the ECF changes ADH Secretion Increases Recall of Fluids The secretion of ADHrestricts water loss andstimulates thirst, promotingadditional waterconsumption. Because the ECFosmolarity increases,water shifts out of the ICF, increasing ECFvolume and lowering ECF Na concentrations. Rising plasmasodium levels Osmoreceptorsin hypothalamusstimulated HOMEOSTASISRESTORED HOMEOSTASISDISTURBED If you consume largeamounts of salt withoutadequate fluid, as whenyou eat salty potatochips without taking a drink, the plasma Naconcentration rises temporarily. Decreased Nalevels in ECF Increased Nalevels in ECF HOMEOSTASIS Start Normal Naconcentrationin ECF
Figure 24.3 1 The mechanisms that regulate sodium balancewhen sodium concentration in the ECF changes HOMEOSTASIS Start Normal Naconcentrationin ECF HOMEOSTASISDISTURBED HOMEOSTASISRESTORED Decreased Nalevels in ECF Increased Nalevels in ECF Water loss reducesECF volume,concentrates ions Osmoreceptorsin hypothalamusinhibited ADH SecretionDecreases As soon as the osmoticconcentration of the ECFdrops by 2 percent ormore, ADH secretiondecreases, so thirst issuppressed and waterlosses at the kidneysincrease. Falling plasmasodium levels
Module 24.3: Water and sodium balance Sodium balance (continued) Exchange changes in Na+ are accommodated by changes in blood pressure and volume Hyponatremia (natrium, sodium) Low ECF Na+ concentration (<136 mEq/L) Can occur from overhydration or inadequate salt intake Hypernatremia High ECF Na+ concentration (>145 mEq/L) Commonly from dehydration
Module 24.3: Water and sodium balance Sodium balance (continued) Exchange changes in Na+ are accommodated by changes in blood pressure and volume (continued) Increased blood volume and pressure Natriuretic peptides released Increased Na+ and water loss in urine Reduced thirst Inhibition of ADH, aldosterone, epinephrine, and norepinephrine release Decreased blood volume and pressure Endocrine response Increased ADH, aldosterone, RAAS mechanism Opposite bodily responses to above
Figure 24.3 2 The mechanisms that regulate water balancewhen ECF volume changes Responses to Natriuretic Peptides Combined Effects Increased Na loss in urine Reduced bloodvolume Increased water loss in urine Rising bloodpressure andvolume Natriuretic peptidesreleased by cardiacmuscle cells Reduced thirst Reduced bloodpressure Inhibition of ADH, aldosterone,epinephrine, and norepinephrinerelease Increased bloodvolume andatrial distension HOMEOSTASISRESTORED HOMEOSTASISDISTURBED Falling ECF volume Rising ECF volume by fluidgain or fluid and Na gain HOMEOSTASIS Start Normal ECFvolume
Figure 24.3 2 The mechanisms that regulate water balancewhen ECF volume changes HOMEOSTASIS Start Normal ECFvolume HOMEOSTASISDISTURBED HOMEOSTASISRESTORED Falling ECF volume by fluidloss or fluid and Na loss Rising ECF volume Decreased bloodvolume andblood pressure Endocrine Responses Combined Effects Increased renin secretionand angiotensin IIactivation Increased urinary Na retention Decreased urinary water loss Increased aldosteronerelease Increased thirst Falling bloodpressure andvolume Increased ADH release Increased water intake
Module 24.3 Review a. What effect does inhibition of osmoreceptors have on ADH secretion and thirst? b. What effect does aldosterone have on sodium ion concentration in the ECF? c. Briefly summarize the relationship between sodium ion concentration and the ECF.
CLINICAL MODULE24.4: Potassium imbalance Potassium balance (K+ gain = loss) Major gain is through digestive tract absorption ~100 mEq (1.9–5.8 g)/day Major loss is excretion by kidneys Primary ECF potassium regulation by kidneys since intake fairly constant Controlled by aldosterone regulating Na+/K+ exchange pumps in DCT and collecting duct of nephron Low ECF pH can cause H+ to be substituted for K+ Potassium is highest in ICF due to Na+/K+ exchange pump ~135 mEq/L in ICF vs. ~5 mEq/L in ECF
Figure 24.4 1 The major factors involved in potassium balance Factors Controlling Potassium Balance Approximately 100mEq (1.9–5.8 g) ofpotassium ions are absorbed by thedigestive tract eachday. Roughly 98 percent of thepotassiumcontent of thehuman body is inthe ICF, ratherthan the ECF. The K concentration in theECF is relatively low. The rateof K entry from the ICFthrough leak channels isbalanced by the rate of Krecovery by the Na/Kexchange pump. When potassiumbalance exists,the rate of urinaryK excretionmatches the rateof digestive tractabsorption. The potassium ionconcentration in theECF is approximately5 mEq/L. KEY Absorption The potassium ionconcentration of theICF is approximately135 mEq/L. Renal K lossesare approximately100 mEq per day Secretion Diffusion through leak channels
Figure 24.4 2 The role of aldosterone-sensitive exchange pumpsin the kidneys in determining the potassiumconcentration in the ECF The primary mechanism ofpotassium secretion involvesan exchange pump thatejects potassium ions whilereabsorbing sodium ions. Tubularfluid ECF The sodium ions are then pumped outof the cell in exchange for potassiumions in the ECF. This is the same pumpthat ejects sodium ions entering thecytosol through leak channels. KEY Aldosterone- sensitive exchange pump Sodium-potassium exchange pump
Figure 24.4 3 Events in the kidneys that affect potassium balance Under normal conditions, thealdosterone-sensitive pumpsexchange K in the ECF forNa in the tubular fluid. Thenet result is a rise in plasmasodium levels and increasedK loss in the urine. Distalconvolutedtubule When the pH falls in the ECFand the concentration of H isrelatively high, the exchangepumps bind H instead of K.This helps to stabilize the pHof the ECF, but at the cost ofrising K levels in the ECF. Collectingduct
Disturbances of potassium balance Hypokalemia (kalium, potassium) Below 2 mEq/L in plasma Can be caused by: Diuretics Aldosteronism (excessive aldosterone secretion) Symptoms Muscular weakness, followed by paralysis Potentially lethal when affecting heart CLINICAL MODULE24.4: Potassium imbalance
Disturbances of potassium balance (continued) Hyperkalemia Above 8 mEq/L in plasma Can be caused by: Chronically low pH Kidney failure Drugs promoting diuresis by blocking Na+/K+ pumps Symptoms Muscular spasm including heart arrhythmias CLINICAL MODULE24.4: Potassium imbalance
CLINICAL MODULE24.4 Review a. Define hypokalemia and hyperkalemia. b. What organs are primarily responsible for regulating the potassium ion concentration of the ECF? c. Identify factors that cause potassium excretion.
Section 2: Acid-Base Balance Learning Outcomes 24.5Explain the role of buffer systems in maintaining acid-base balance and pH. 24.6 Explain the role of buffer systems in regulating the pH of the intracellular fluid and the extracellular fluid. 24.7 Describe the compensatory mechanisms involved in the maintenance of acid-base balance. 24.8 CLINICAL MODULE Describe respiratory acidosis and respiratory alkalosis.
Section 2: Acid-Base Balance Acid-base balance (H+ production = loss) Normal plasma pH: 7.35–7.45 H+ gains: many metabolic activities produce acids CO2 (to carbonic acid) from aerobic respiration Lactic acid from glycolysis H+ losses and storage Respiratory system eliminates CO2 H+ excretion from kidneys Buffers temporarily store H+
Figure 24 Section 2 1 The major factors involved in the maintenanceof acid-base balance The respiratory systemplays a key role byeliminatingcarbon dioxide. The kidneys play a majorrole by secretinghydrogen ions into the urine and generatingbuffers that enter thebloodstream. The rate ofexcretion rises and fallsas needed to maintainnormal plasma pH. As a result, the normal pH ofurine varies widely butaverages 6.0—slightlyacidic. Active tissuescontinuously generatecarbon dioxide, which insolution forms carbonicacid. Additional acids,such as lactic acid, areproduced in the course ofnormal metabolicoperations. Normalplasma pH(7.35–7.45) Tissue cells Buffer Systems Buffer systems cantemporarily store Hand thereby provideshort-term pHstability.
Section 2: Acid-Base Balance Classes of acids Fixed acids Do not leave solution Remain in body fluids until kidney excretion Examples: sulfuric and phosphoric acid Generated during catabolism of amino acids, phospholipids, and nucleic acids Organic acids Part of cellular metabolism Examples: lactic acid and ketones Most metabolized rapidly so no accumulation
Section 2: Acid-Base Balance Classes of acids (continued) Volatile acids Can leave body by external respiration Example: carbonic acid (H2CO3)
Module 24.5: Buffer systems pH imbalance ECH pH normally between 7.35 and 7.45 Acidemia (plasma pH <7.35): acidosis (physiological state) More common due to acid-producing metabolic activities Effects CNS function deteriorates, may cause coma Cardiac contractions grow weak and irregular Peripheral vasodilation causes BP drop Alkalemia (plasma pH >7.45): alkalosis (physiological state) Can be dangerous but relatively rare
Figure 24.5 2 The narrow range of normal pH of the ECF, and the conditions that result from pH shifts outside the normal range The pH of the ECF(extracellular fluid)normally ranges from7.35 to 7.45. When the pH of plasma falls below7.5, acidemia exists. Thephysiological state that results iscalled acidosis. When the pH of plasma risesabove 7.45, alkalemia exists.The physiological state thatresults is called alkalosis. Extremelyacidic Extremelybasic pH Severe acidosis (pH below 7.0) can be deadlybecause (1) central nervous system functiondeteriorates, and the individual may becomecomatose; (2) cardiac contractions grow weak andirregular, and signs and symptoms of heart failuremay develop; and (3) peripheral vasodilationproduces a dramatic drop in blood pressure,potentially producing circulatory collapse. Severe alkalosis is alsodangerous, but serious casesare relatively rare.
Module 24.5: Buffer systems CO2 partial pressure effects on pH Most important factor affecting body pH H2O + CO2 H2CO3 H+ + HCO3– Reversible reaction that can buffer body pH Adjustments in respiratory rate can affect body pH
Figure 24.5 3 The inverse relationship between the PCO2 and pH PCO240–45mm Hg pH7.35–7.45 HOMEOSTASIS If PCO2 rises If PCO2 falls H2CO3 H2CO3 H2O CO2 H2O CO2 H HCO3 H HCO3 When the PCO2 falls, the reaction runs in reverse, andcarbonic acid dissociates into carbon dioxide andwater. This removes H ions from solution andincreases the pH. When carbon dioxide levels rise, more carbonic acidforms, additional hydrogen ions and bicarbonate ionsare released, and the pH goes down. pH PCO2 PCO2 pH
Module 24.5: Buffer systems Buffer Substance that opposes changes to pH by removing or adding H+ Generally consists of: Weak acid (HY) Anion released by its dissociation (Y–) HY H+ + Y– and H+ + Y– HY
Figure 24.5 4 H HY H H Y HY H Y H Y H HY H The reactions that occur when pH buffer systems function Adding H to thesolution upsets the equilibrium and resultsin the formation ofadditional molecules ofthe weak acid. Removing H from thesolution also upsets theequilibrium and results in the dissociation ofadditional molecules ofHY. This releases H. A buffer system in body fluids generallyconsists of a combination of a weak acid (HY) and the anion (Y) released by its dissociation.The anion functions as a weak base. In solution,molecules of the weak acid exist in equilibriumwith its dissociation products.
Module 24.5 Review a. Define acidemia and alkalemia. b. What is the most important factor affecting the pH of the ECF? c. Summarize the relationship between CO2 levels and pH.
Module 24.6: Major body buffer systems Three major body buffer systems All can only temporarily affect pH (H+ not eliminated) Phosphate buffer system Buffers pH of ICF and urine Carbonic acid–bicarbonate buffer system Most important in ECF Fully reversible Bicarbonate reserves (from NaHCO3 in ECF) contribute
Module 24.6: Major body buffer systems Three major body buffer systems (continued) Protein buffer systems (in ICF and ECF) Usually operate under acid conditions (bind H+) Binding to carboxyl group (COOH–) and amino group (—NH2) Examples: Hemoglobin buffer system CO2 + H2O H2CO3 HCO3– + Hb-H+ Only intracellular system with immediate effects Amino acid buffers (all proteins) Plasma proteins
Figure 24.6 1 The body’s three major buffer systems Buffer Systems occur in Intracellular fluid (ICF) Extracellular fluid (ECF) Carbonic Acid–Bicarbonate Buffer System Phosphate BufferSystem Protein Buffer Systems Contribute to the regulation of pH in the ECF and ICF;interact extensively with the other two buffer systems Has an importantrole in buffering thepH of the ICF andof urine Is most important in theECF Amino acidbuffers(All proteins) Plasmaproteinbuffers Hemoglobinbuffer system(RBCs only)
Figure 24.6 4 BICARBONATE RESERVE The reactions of the carbonic acid–bicarbonate buffer system Body fluids contain a large reserve ofHCO3, primarily in the form of dissolvedmolecules of the weak base sodiumbicarbonate (NaHCO3). This readilyavailable supply of HCO3 is known asthe bicarbonate reserve. CARBONIC ACID–BICARBONATEBUFFER SYSTEM NaHCO3(sodium bicarbonate) CO2 H2CO3(carbonic acid) H CO2 H2O HCO3 HCO3 Na (bicarbonate ion) Lungs The primary function of the carbonicacid–bicarbonate buffer system is toprotect against the effects of the organicand fixed acids generated throughmetabolic activity. In effect, it takes the Hreleased by these acids and generatescarbonic acid that dissociates into waterand carbon dioxide, which can easily be eliminated at the lungs. Addition of Hfrom metabolicactivity Start