An Introduction to Chest X-rays
210 likes | 586 Vues
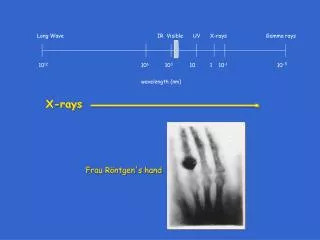
An Introduction to Chest X-rays. Dr Sam Carvey FY2 N.M.G.H. Why request a CXR?. SOB Chest pain Chronic cough Trauma Line insertion NG/NJ tube. Normal CXR . 11. 1. 3. 7. 7. 6. 2. 5. 4. 9. 8. 12. 10. Trachea Right Atrium Aortic knuckle Left ventricle Lung fields

An Introduction to Chest X-rays
E N D
Presentation Transcript
An Introduction to Chest X-rays Dr Sam Carvey FY2 N.M.G.H.
Why request a CXR? • SOB • Chest pain • Chronic cough • Trauma • Line insertion • NG/NJ tube
Normal CXR 11 1 3 7 7 6 2 5 4 9 8 12 10
Trachea • Right Atrium • Aortic knuckle • Left ventricle • Lung fields • Horizontal fissure • Hilum • Diaphragm • Cardiophrenic angle • Costophrenic angle • Apex • Anterior rib
Lateral CXR • Used to localise lesions/pathology seen on frontal XR. In practice never requested! • In theory good to have basic understanding as helps to understand lobes. • Might come up in an exam to throw you
Trachea • Right ventricle • Left ventricle • Left atrium • Hilum • Aorta 1 4 5 6 2 Horizontal fissure 3 Right oblique Left oblique
What makes a good CXR? 1. PA vs AP • PA is the most accurate. This stands for posterior to anterior. X-ray beams are aimed from behind patient to cassette in front from a distance of approx 180cm. This results in minimally divergent beams. • Requires patient to stand in front of cassette therefore can be difficult for some patients. • AP (anterior to posterior) films are taken when patient is too unwell/frail to stand for PA. • On AP films the mediastinum in magnified (as heart is further away from the cassette and closer to the beams) • Portable/bedside XRs are always AP. The are also compromised as patient often cannot take full inspiration or may be rotated. The beam is never going to be 180cm away!
2. Inspiration • XR’s should be take during inspiration • General rule is 6 anterior ribs above the diaphragm. Shallow inspiration Causes: • Pain • frail/elderly • unconscious Problems: • transverse cardiac diameter may appear artificially large • Vessels can appear crowded at lung bases giving a false appearance of infection/collapse
3.Exposure • Vertebral bodies should just be visible through lower part of cardiac shadow. • If you cannot see them the film is underpenetrated. Lung fields will appear falsely white. • If they are too clearly visible the film is overpenetrated. 4. Rotation • Medial end of each clavicle should be equal distance from centre of vertebrae. • Rotation can make manubrium/aorta/vessels appear more prominent. This could simulate a mass/mediastinal widening. 5. Scapula • Arms should be abducted to remove scapula from picture.
Method to interpreting a CXR • Be systematic. • Sometimes best to comment on a blatantly obvious abnormality first if you are confident then start with your system. • Don’t forget the boring bits – name, type, quality of the film – especially in the exams!
Descriptive terms • Upper, middle, lower zone • Zones if you’re sure you know which one but often impossible from PA alone • Shadowing • dense, fluffy, diffuse, nodular, reticular, linear • Lucency - black • Opaque - white • Consolidation • Means a pathological process that fills the alveoli with pus/blood/fluid/cells etc • Most commonly infection • Pneumonia and consolidation are often used synonymously but not strictly true. • Probably best to say “an area of consolidation most likely to represent infection” • Silhouette sign • An intrathoracic lesion touching a border of the heart/aorta/diaphragm will obliterate that border on CXR. • Air bronchogram • Tubular outline of bronchus. • Usually pneumonia
System Example: • Introduction • Trachea • Lungs • Hilum • Heart and mediastinum • Diaphragm • Bones and soft tissues • Forgotten areas
Introduction • Name (if you know it / it is on the film) • Age • Male or female? - In the exam you might not actually have this info but watch out for breast shadows as the examiner might want you to comment on this. • Date • Type of film (AP, PA, Supine, Portable, Erect) • Quality (penetration, inspiration, rotation, scapula withdrawn) So a good opening statement is: “This is a PA chest radiograph of Jane Bloggs, taken on the 8/03/11. The penetration is adequate, the patient has taken a good inspiration and does not appear rotated”
2. Trachea • Should be central. Deviation can indicate lung pathology • Towards affected side – collapse • Away from affected side – mass, pneumothorax, pleural effusion 3. Lung fields • Should be equal transradiancy. • Look for shadows (discrete, generalised, consolidation, collapse, effusion) • Increased translucency? (think pneumothorax, bulla, hyperinflation, pulmonary embolism, caviating mass) • Increased opacity? ( think collapse, consolidation, effusion, lesion) • Check cardiophrenic and costophrenic angles and apex. • Horizontal fissure • Fissure between upper and lower lobe on right. Should run from hilum to axilla, approx 6th rib. Not always seen. Change in position can indicate pathology (eg. collapse) • Pleura - Check lung markings run to costal edge -?pneumothorax
4. Hilum • Composed of pulmonary arteries, veins, lymph nodes and airways • Position • Left is slightly higher than right in majority. Occasionally equal. Right should not be higher than left. Is the hilum in an abnormal place? (eg.pulled up/down by collapse • Shape and density • Should be concave and similar appearance bilaterally. Enlarged =?HF Bulky =?mass 5. Mediastinum • Check for clear edge • Should be 30% or less intrathoracic diameter. • Enlarged? Think aortic dissection, lymph nodes, thymus, thyroid, tumour
Heart • Cardiothoracic ratio should be less than 50%. • ?enlarged – think heart failure, cardiomyopathy, pericardial effusion • Is the shape normal? • Ventricular aneursym? Dilated/hypertrophied atrium/ventricle? 6. Diaphragms • Position. • Right diaphragm should be higher than left by approx 3cm although this is very variable. • Elevated or depressed? Why? Is something pushing it down or pulling it up? • Check for free air under the diaphragm • Are they clearly defined? If not why? – mass? Pneumonia?
7. Bones • Fractures • - Fractures in clavicle/ribs could cause pneumo/haemothorax! • Unusual looking bone • - ?metastases • Soft tissues • Breast shadows • Subcutaneous fat • Surgical emphysema • 8. Frequently forgotten areas! • Apex • - TB? Pancoasts tumour? • Behind the heart • - Malignancy? • Under the diaphragm • - Free air!!
Elizabeth Duke 17/03/1976 03/03/2011 PA
Frank Butcher 04/05/1944 11/01/2011 AP