Coronary Heart Disease
440 likes | 1.28k Vues
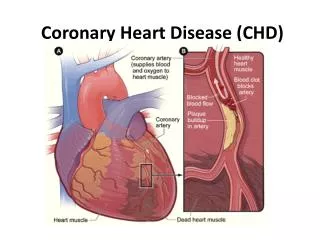
Coronary Heart Disease. Pericarditis. Acute infectious pericarditis Either dry or exudative Exudative: restricts cardiac filling and emptying, decreases cardiac output and tissue perfusion Chronic constrictive pericarditis

Coronary Heart Disease
E N D
Presentation Transcript
Pericarditis • Acute infectious pericarditis • Either dry or exudative • Exudative: restricts cardiac filling and emptying, decreases cardiac output and tissue perfusion • Chronic constrictive pericarditis • Fibrosis of the pericardial sac; pericardial layers adhere to each other. • Causes scarring and thickening of pericardium. • Decreases cardiac filling and contracting. • Leads to decreased cardiac output and heart failure.
Pericarditis – Clinical Manifestations • Bacterial pericarditis • Onset • High Fever • Flu like • Symptoms • Leukocytosis • Increased ESR • Anorexia, weight loss • Acute stages • Weight loss, anorexia, nausea
Pericardial Effusion -Treatment • Anti-inflammatory Medications • Invasive Procedures • Pericardiocentesis • Open Heart Surgery • Intrapericardial Sclerosis • Pericardiectomy
Pulmonary Edema • Extreme shortness of breath or difficulty breathing • A feeling of suffocating or drowning • Wheezing or gasping for breath • Anxiety, restlessness or a sense of apprehension • A cough that produces frothy sputum that may be tinged with blood • Excessive sweating • Pale skin • Palpitations
Cardiac Tamponade Cardiac tamponade can occur due to: • Dissecting aortic aneurysm (thoracic) • End-stage lung cancer • Acute MI • Heart surgery • Pericarditis bacterial or viral infections • Wounds to the heart
Defibrillation • Defibrillation is a process in which an electronic device gives an electric shock to the heart. • Re-establishes normal contraction rhythms in a heart having dangerous arrhythmia or in cardiac arrest.
Pacemaker • Single-Chamber Pacemakers: Only one wire (pacing lead) is placed into a chamber of the heart. • Dual-Chamber Pacemakers: Wires are placed in two chambers of the heart. One lead paces the atrium and one paces the ventricle.
Pacemaker • Rate-Responsive Pacemakers: Sensors automatically adjust to changes in a person's physical activity. • Other devices: Such as implantable cardioverter defibrillators designed primarily for other purposes, can function as pacemakers in certain situations.
Cardiac Ablation • Atrial Fibrillation • Atrial Flutter • AV Nodal Reentrant Tachycardia • AV Reentrant Tachycardia • Atrial Tachycardia • Risk Factors • Bleeding • Puncture of the heart • Damage to heart's electrical system • Blood clots • Pulmonary vein stenosis • Kidney damage
Cardiac Resynchronization Therapy (CRT) • The ideal candidate for a CRT device is someone with: • Moderate to severe CHF symptoms, despite lifestyle changes and medication . • A weakened and enlarged heart muscle . • A significant electrical delay in the lower pumping chambers (bundle branch block).
Cardioversion • NPO at least eight hours prior to the procedure. • Informed Consent • Take regularly scheduled medications before the procedure. • Diabetics need to discuss dosing prior to the procedure. • Patient should bring a list of all medications • No lotions or ointments to chest or back as this may interfere with the adhesiveness of the shocking pads. • No jewelry on chest.
Sudden Cardiac Death (SCD) • SCD causes half of all heart disease deaths. • In SCD, electrical problems keep the heart from pumping the right way, when suddenly, the heart stops working. • Treating someone in SCD requires “paddles” to shock the heart. • FYI…In a heart attack, a blockage in blood vessels slows or stops blood flow.
Dilated Cardiomyopathy • Most often follows MI and ventricular tissue remodeling • Coronary artery disease is most common cause in US patients • Up to 30% of cases have genetic cause • Numerous risk factors may precipitate • 50% of cases lack identifiable cause
Left Ventricular Assist Device (LVAD) • Waiting for a heart transplant • Hearts function can become normal again • Not a good candidate for a heart transplant Risks: • Blood Clots • Bleeding • Infection • Device malfunction • Right heart failure
Cardiac Transplantation • Reasons for Transplant: • Coronary artery disease • Cardiomyopathy • Valvular heart disease • Congenital heart defect • Failure of a previous heart transplant • Risk Factors • Medication Side Effects • Cancer • Infection
Nursing Management • Clinical status and procedure dictate patient management. • Patients NPO at least 6 hours. • Complete assessment before procedure including when meds were last taken. • Pretreat patients with history of anaphylactic reaction to contrast dye.
Nursing Management Discharge criteria include: • Stable vital signs • Review DASH for Hypertension • Increase in calcium and decrease in sodium. • No evidence of complications at access site • Ability to ambulate without assistance. • Voiding without difficulty
Dilated Cardiomyopathy • Most often follows MI and ventricular tissue remodeling. • Coronary artery disease is more common cause in US patients. • Up to 30% of cases have genetic cause. • Numerous risk factors may precipitate • 50% of cases lack identifiable cause.
Dilated Cardiomyopathy – Nursing Management • Detailed history • In-depth physical assessment of effect on ability to perform ADLs • Identify risk factors/diseases that mimic DCM • Care plan: conserve energy, decrease heart’s workload via paced or reduced activity, positioning, oxygen therapy
Hypertrophic Cardiomyopathy (HCM) • Disorder of sarcomere (contractile element of cardiac muscle) • Characterized by left (and occasionally right) ventricular hypertrophy, also hypertrophy in septum
Hypertrophic Cardiomyopathy Nursing Management • Assess/monitor progress of disease (hemodynamic status and cardiac output) • Educate about hydration, prophylactic antibiotics, exercise and activity restriction • Identify and help alleviate potential stressors • Provide ‘realistic hope’ and emotional support
Restrictive Cardiomyopathy (RCM) • Least common type in US • Characterized by endocardial scarring • Usually affects one or both ventricles • Restricts filling of blood • Results in systolic dysfunction • No specific treatment or cure
Restrictive Cardiomyopathy – Nursing Management • Decrease workload of heart, conserve energy. • Teach patient to avoid situations that impair venous filling or lower cardiac output.
Hypertensive Crisis Urgent • Increased blood pressure • Severe headache • Severe anxiety • Shortness of breath Emergent • Fluid in your lungs • Brain swelling or bleeding • Aortic dissection • Heart attack • Stroke • High blood pressure with seizures (eclampsia), if pregnant
Aortic Dissection Standford Classification System A – Originated and involves ascending aorta B – Originated and involves descending aorta
Aortic Dissection Typical signs and symptoms include: • Sudden severe chest or upper back pain, often described as a tearing, ripping or shearing sensation, that radiates to the neck or down the back • Loss of consciousness • Shortness of breath • Weakness or paralysis • Stroke • Sweating • High blood pressure • Different pulse rates in each arm
Hemodynamic Monitoring • Afterload • Cardiac Index • Cardiac Output • Central venous Pressure • Mean Arterial Pressure • Preload
Hemodynamic Monitoring • Pulmonary Artery Pressure • Pulmonary Capillary Wedge Pressure • Pulmonary Vascular Resistance • Right Ventricular Pressure • Stroke Index • Stroke Volume • Systemic Vascular Resistance
Type I Antiarrhythmics: Sodium Channel Blockers • Class 1A: Disopyramide (Norpace, NAPAmide), Procainimide (Procanbid), Quinidine (APO Quinidine) • Class 1B: Lidocaine (Xylocaine), Mexiletene (Mexitel), • Class 1C: Flecainide (Tambocor)
Type II Antiarrhythmics: Beta-Adrenergics or Beta Blockers • Atenolol (Tenormin) • Esmolol (Brevibloc) • Toptol (Metoprolol) • Lopressor (Metoprolol) • Nadolol (Corgard) • Propranolol (Inderal) • Acebutolol (Sectral)
Type III Antiarrhythmics: Potassium Channel Blockers • Amiodarone (Cordarone, Pacerone) • Bretylium, Sotalol (Betapace) • Ibutilide (Corvert) • Dofetilide (Tikosyn)
Type IV Antiarrhythmics: Calcium Channel Blockers Amlodipine (Norvasc) Verapamil (Calan) Nifedipine, (Procardia) Nicardipine (Cardene) Diltiazem (Cardizem, Tiazac)
Angiotensin Converting Enzyme • Benazepril (Lotensin) • Captopril (Capoten) • Enalapril (Vasotec) • Lisinopril (Zestril, Prinivil) • Quinapril (Accupril) • Ramipril (Altace) • Trandolapril (Mavik)
Angiotensin II Receptor Antagonists • Candesartan (Atacand) • Eprosartan (Teveten) • Irbesartan (Avapro) • Losartan (Cozaar) • Olmesartan (Benicar) • Telmisartan (Micardis) • Valsartan (Diovan)
Alpha-Adrenergic Blockers (Alpha Blockers) • Doxazocin (Cardura) • Prazosin (Minipress) • Alfuzosin (Uroxatral) • Terazocin (Hytrin) • Tamsulosin (Flomax)
Diuretics Thiazides: Chlorothiazide (Diuril), Hydrochlorothiazide (Microzide), Indapramine (Lozol), Metolazone (Zaroxolyn) Loop: Bumetanide (Bumex) Furosemide (Lasix) Ethacrynic acid (Edecrin), Torsemide (Demadex) Potassium Sparing: Amiloride (Midamor), Spironolactone (Aldactone) , Triamterene (Dyrenium), Eplereone (Inspra)