Download

1 / 48
480 likes | 566 Vues
Tackling Coronary Heart Disease. Inequality in CHD services health outcomes how much? What is to be done?. Population public health interventions.

E N D
Inequality in CHD services health outcomes how much? What is to be done? Population public health interventions
What conclusions can be drawn from the HLPI data about inequalities in service provision and health outcomes for CHD, across Northern and Yorkshire?
What are HLPIs? • Higher Level Performance Indicators • Values attributed to each Health Authority in England, recording their performance in various parameters • Adjusted for age and sex • NOT adjusted for social and economic characteristics of a population
Accessing HLPIs • www.doh.gov.uk.nhsperformanceindicators/index.htm • Deaths from all Deaths from all Deaths from Deaths from Suicides Deaths from Accident Morbidity • causes age 15-64 causes age 65-74 cancer circulatory diseases accidents • Specification Specification Specification Specification Specification Specification Specification • ENGLAND 89 87 137 133.8 9.2 16.4 314.4 • Avon 78 75 123.4 115 7.4 15 345.5 • Barking and 89 87 150.8 136.1 5.7 14.9 293.3 • Havering • Barnet 71 74 115.7 108.3 7.7 11.8 232.9 • Barnsley 107 107 158.3 167.4 11.4 13.4 407.6 • Bedfordshire 84 81 130.2 123.5 8 19.8 273.1
Purpose of HLPIs • allow comparisons to be made between different Health Authorities and NHS trusts • reflect key Government priorities • highlight areas of inequality, to be addressed by the National Plan
Drawbacks of HLPIs • Difficulty interpreting the data as presented on the website • Not direct measures of quality • Differing data collection methods • Values are averages for each HA • Do not assess coping vs demand • Misleading if examined alone
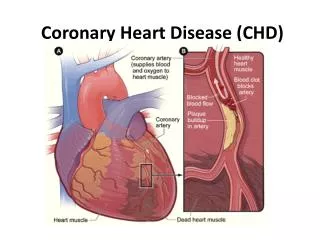
CHD parameters • Deaths from all circulatory diseases (under 75 years only) • Surgery rates for CHD • Deaths in hospital within 30 days of admission for a heart attack (35-74 years only)
Deaths from all circulatory diseases by Health Authority - 1996-98Age/sex standardised rate per 100,000 persons aged under 75
Deaths in hospital within 30 days following a heart attack by Health Authority - 1996-98Age/sex-standardised rate per 100,000 persons aged 35-74 years
Revascularisation rate by Health AuthorityAge-standardised rate per 100,000 persons aged under 75 years, 1996-98
CHD trends in England from 1997-1999 • twofold variation in the death rate from all circulatory disease between the worst and best Health Authorities • whilst there was a 9% increase between 1997/98 and 1998/99 in the elective surgery rates for CABG/PTCA, one third of all Health Authorities saw no increase at all
CHD trends in the Northern and Yorkshire region • all except N. Yorkshire of the 13 DHA are above the England average for deaths from circulatory diseases, with 8 appearing in the top 24 • 10 DHA are below the England average for deaths in hospital within 30 days of admission for a heart attack • 9 DHA are above England average for revascularisation rates, but only Tees is nearing the 1500/million NSF goal
Revascularisation rate and circulatory disease death rate for all Health Authorities in EnglandAge/sex standardised rate per 100,000 persons aged under 75 years, 1996-98
Revascularisation rate and circulatory disease death rate for Northern and Yorkshire regionAge/sex standardised rate per 100,000 persons under 75 years, 1996-98 • some correlation between death rate and revascularisation rate • high circulatory disease death rates for all Health Authorities within Northern and Yorkshire
Association between average distance travelled for revascularisation and revascularisation rate by Health Authority in England, 1996-98
Townsend deprivation score • 4 indicators used to assess level of deprivation • Unemployment - percent of economically active residents aged 16-59/64 who are unemployed • Car ownership - percent of private households who do not possess a car • Home ownership - percent of private households not owner occupied • Overcrowding - percent of private households with more than one person per room • the higher the score, the higher the level of deprivation
Deaths from circulatory disease against Townsend deprivation score for England - 1996-98Age/sex standardised rate per 100,000 persons under 75 years
Circulatory disease deaths and Townsend deprivation score for Northern and Yorkshire region 1996-98 • positive correlation between death from circulatory disease and Townsend deprivation score • no significant correlation found between death within 30 days following AMI or surgery rate and Townsend deprivation scores
Conclusion • inequalities within England and Northern and Yorkshire region for CHD • poorer health outcomes in Northern and Yorkshire region for CHD • provision of services for CHD is more in line with need in Northern and Yorkshire region than England • difficult to interpret HLPI
What is an NSF? • Key tool for tackling major health issues and important diseases. • Aims to improve health, reduce inequalities and raise the quality of care. • Sets of a vision for the future. • Will evolve over time.
Why does CHD need targeting? • Every year >1.4 million people suffer from angina. • 300,000 people have heart attacks each year • 135,000 patients die of heart problems. • 35 million days are lost each year due to CHD. • Inequalities in prognosis.
CHD 22% CHD All All causes causes 78% CHD as a proportion of deaths from all causes in England and Wales in 1998
NSF for CHD • Published in March 2000 • Aimed at transforming the prevention, diagnosis and treatment of CHD. • Ensures services are available to everyone who can benefit. • Over a ten year period will save 20,000 lives/year. • Sets out 12 standards of system reform and expansion.
Principles underpinning the NSF. • Reducing the burden of CHD requires action across society, not just the NHS. • Quality of care depends on: • access to appropriate services • interaction between clinicians and patients. • Quality of the organisation and environment. • Simple things done at the right time. • Structured and systematic care.
Making it happen. • Local health communities and delivery plans. • National and regional systems and strategies to support this. • National CHD implementation group. • Regional offices of the NHSE to monitor performance.
Health Outcomes • NSF established 12 standards for • prevention • diagnosis • treatment of CHD • Remain relevant for 10 years (or more!)
Standards • Reduce heart disease in the population • reduce prevalence of risk factors • reduce inequalities of risk factors • reduce prevalence of smoking • Prevent CHD in high risk patients • identify people with established CHD • identify people at significant risk
Heart attack and other acute coronary syndromes • receive expert help within 8 minutes of calling for help • assessed professionally, and receive aspirin • protocols be put in place by NHS trusts
Stable angina • receive appropriate investigations and treatment
Stable angina • receive appropriate investigations and treatment • Revascularisation • urgent referral to cardiologist • hospital-wide system of care
Heart failure • appropriate investigations or alter diagnosis • identify cause and treat • Cardiac rehabilitation • multidisciplinary programme offered
Inequality in CHD services health outcomes how much? What is to be done? Population public health interventions
Services Population Smoking cessation High risk prevention Primary care clinics Acute coronary syndromes Quick hospital care Stable angina Ix and Rx protocols Protocols for Ix Targets for Rx Revascularisation Community support Dedicated hospital clinics Heart failure Lifestyle interventions Education Rehabilitation
Inequalities • Resources • Health Action Zones Primary Care Trusts shifting the balance of power • Prevention or cure? • Re-enforcing inequalities? • Evaluation
The NSF has a strong NHS focus to tackling CHD. What wider public health initiatives might improve CHD health outcomes at a population level?
Saving Lives:Our Healthier Nation Target: to reduce the death rate from coronary heart disease and stroke and related diseases in people under 75 years by at least two fifths by 2010-saving up to 200,000 lives in total
Smoking Kills: White paper • reduce illegal sales of cigarettes • monitor the advertising ban • encourage media advocacy • reduce smoking in public places • work to support any national media campaigns • develop smoking cessation services.
Smoking cessation services • identify smoking status of patients • provide advice and info on NRT • access to smoking cessation services including back-up of intensive services • provision of NRT, free for one week to poorer smokers • Don’t Give Up Giving Up
Specialist Health Promotion Services • Smoking Cessation Services Number of people setting a quit date 2284 Number of people quit at 4weeks 1260 Number of people not quit at 4weeks 599 Number of people not known/lost to 425 follow up • Target for 2000/2001 546
Healthy diet • National School Fruit Scheme • Five-a-day programme • work with food industry • a reform of the welfare foods programme • hospital nutrition policy • involvement of family and friends
Physical inactivity • regular exercise • aim to encourage adults to build into daily routine, half an hour of moderate exercise • prevent or delay hypertension • control diabetes and regulate weight
Physical inactivity • promotes safe, healthy travel to school • National Healthy Schools Standard which includes physical activity • Exercise referral • Health Walk Programme
Overweight/obesity • for overweight people(BMI 25+) or obese(30+), a 10% weight loss can confer significant health benefits • central obesity gives higher risk • dietary advice combined with physical activity • support
Summary • Government cannot succeed through its actions alone. It needs to work in partnership with local players such as the NHS, local authorities, schools and employers.