Download
1 / 70
700 likes | 1.11k Vues
The Adrenal. Adrenal Anatomy. Composed of a cortex and medulla , which have separate embryology. Adrenal Anatomy. The adrenal cortex arises fro m the coelomic mesoderm between the fourth and sixth weeks of gestation. Adrenal Anatomy.

E N D
Adrenal Anatomy • Composed of a cortex and medulla, which have separate embryology.
Adrenal Anatomy • The adrenal cortex arises fro m the coelomic mesoderm between the fourth and sixth weeks of gestation.
Adrenal Anatomy • The adrenal medulla is derived from cells of the neural crest that also form the sympathetic nervous system and the sympathetic ganglia.Some of these neural crest cells migrate into the adrenal cortex to form the adrenal medulla, but chromaffin tissue may also develop in extraadrenal sites. • The most common site of extraadrenal chromaffin tissue is the organ of Zuckerkandl, located adjacent to the aorta near IMA.
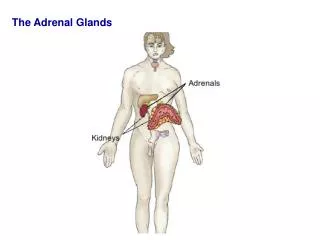
Adrenal Anatomy • The glands weigh about 4g each, located in the retroperitoneum along the superior-medial aspect of the kidneys. • Yellow appearance because of their high lipid content. • 3-5 cm in length, 4-6mm in thickness
Adrenal Anatomy • Left>right • Receive arterial blood from branches of the inferior phrenic artery, aorta, and renal arteries. • The right adrenal vein is short and exits the gland medially to enter the vena cava. The left adrenal vein exits anteriorly and usually drains into the left renal vein. As a result, adrenal venous catheterization is accomplished more easily on the left than the right.
Adrenal Anatomy • The adrenal cortex is composed of three zones histologically. • Outer zona glomerulosa, site for aldosterone synthesis. • Central zona fasciculata and inner zona reticularis produce both cortisol and androgens.
Adrenal Anatomy • Most of the blood supply to the medulla comes from venous blood draining through the cortex. This provides the adrenal chromaffin cells with high concentration of the enzyme phenyethanolamine N- methyltransferase (PNMT) required for conversion of norepinephrine to epinephrine.
The Cortex • Three major hormones • Cortisol • Androgens • Aldosterone
The Cortex • Zona glomerulosa is the exclusive site of production of aldosterone because it lacks the enzyme 17 alpha hydroxylase necessary for production of 17 a- progesterone and 17 a-pregnalone, which are the precursors to cortisol and androgens.
The Cortex • Zona fasciculata and reticularis function as a unit to produce cortisol, androgens, and small amounts of estrogen, but it lacks the enzymes necessary to convert 18-hydroxycorticosterone to aldosterone.
Cortex • Cholesterol is the precursor from which all adrenal steroids are synthesized. • Conversion of cholesterol to pregnenolone is the rate limiting step in adrenal steroidogenesis and is the major site of action of ACTH.
Steroidogenesis Cholesterol Cholesterol desmolase 17α-hydroxylase 17,20 lyase Pregnenolone Progesterone 11-Deoxycorticosterone Corticosterone Aldosterone 17-Hydroxypregnenolone 17-Hydroxyprogesterone 11-Deoxycortisol Cortisol DHEA Androstenedione Testosterone Estradiol 3β hydroxysteroid dehydrogenase 21β-hydroxylase 11β-hydroxylase Aldosterone synthase
Glucocorticoids • Regulated by hypothalamus and pituitary via secretion of CRH and ACTH.
Glucocorticoids • Cortisol, like ACTH is secreted in a pulsitile manner, and plasma levels closely parallel those of ACTH. Superimposed on this is a circadian rhythm that results in peak cortisol levels in the early morning and a nadir in the late evening. • Physical and emotional stress (trauma, surgery, and hypoglycemia) increase cortisol secretion by stimulating release of CRH and ACTH from hypothalamus and pituitary respectively.
Glucocorticoids • Normal daily production of cortisol is 10-30mg. • The liver is the main site of metabolism. Two major metabolites are 17-hydroxycorticosteroids and 17-ketosteroids, excreted in the urine.
Glucocorticoids • Metabolic effects are stimulation of hepatic gluconeogenesis, inhibition of protein synthesis, increased protein catabolism, and lipolysis of adipose tissue.
Glucocorticoids • The increased release of AA from muscle protein and release of glycerol and free fatty acids from fat provide the substrate for hepatic gluconeogenesis. • Also increase glycogen synthesis, peripheral uptake of glucose is inhibited, and may cause hyperglycemia and increased insulin secretion.
Glucocorticoids • Loss of collagen, impair wound healing by inhibition of fibroblasts. • Inhibit bone formation, reduce calcium absorption by gut (steroid induced osteoporosis).
Glucocorticoids • Numerous antiinflammatory actions, which include inhibition of leukocyte mobilization and function, decreased migration of inflammatory cells to sites of injury, decreased production of inflammatory mediators (IL-1, leukotrienes, and bradykinins). • Also essential for cardiovascular stability, as evidenced by the collapse that occurs in patients with adrenal insufficiency.
Androgens • Dehydro-3-epiandrosterone (DHEA) and DHEA sulfate. • Minimal direct biologic activity. • In periphery they undergo conversion to androgens, testosterone, and dihydrotestosterone.
Androgens • Increased in Cushing syndrome, adrenal carcinoma, congenital adrenal hyperplasia. • In adult men accounts for only 5% of testosterone, in prepubertal boys, however, increased production may be manifested by the early development of secondary sexual characteristics and penile enlargement. • In females, manifested by acne, hirsuitism, virilization, and amenorrhea.
Aldosterone • Maintains extracellular fluid volume and regulation of sodium and potassium. • Renin-angiotensin system regulates it.
Aldosterone • Renin is secreted by juxtaglomerular cells of the kidney in response to decreased pressure in the renal afferent arterioles. • Decreased sodium concentration sensed by the macula densa promote renin as well.
Aldosterone • Renin is also stimulated by hyperkalemia, and inhibited by potassium depletion. • Angiotensin II is a potent vasoconstrictor, also stimulates zona glomerulosa to secrete aldosterone. • Aldosterone then stimulates reabsorption ofsodium in exchange for potassium and hydrogen ion secretion.
Cushings Syndrome • Constellation of signs and symptoms that result from chronic glucocorticoid excess. • Most common source is iatrogenic administration of glucocorticoids. • ACTH-secreting tumors of pituitary are the most common cause of spontaneous Cushing syndrome.
Cushing’s Syndrome, Causes Endogenous • Pituitary adenoma (Cushing’s Disease) • Ectopic ACTH production Ectopic CRH production • Adrenal adenoma • Adrenal carcinoma • Adrenal hyperplasia Exogenous • Therapeutic steroids (pills, lotions, creams) • Major depression • Alcoholism
Cushings Syndrome • Pituitary Cushing, also termed Cushing disease, accounts for 70% of all cases of Cushing syndrome. • Ectopic ACTH secreting tumors comprise 15% of all cases and associated with small cell cancers of the lung. • Primary adrenal tumors (adenomas, carcinomas) account for 15-20% of cases.
Cushing Syndrome • These patients lose diurnal variation in cortisol levels. • Elevated levels of urinary free cortisol present in 90% of patients. Normally only 1% of cortisol excreted in urine. • Low dose dexamethasone suppression test will suppress pituitary secretion of ACTH and adrenal production of steroids. So, if am plasma cortisol is suppressed then Cushing is ruled out.
Cushing Syndrome • Plasma ACTH levels are used to differentiate ACTH-dependent (pituitary and ectopic ACTH secreting tumors) from adrenal causes of Cushing syndrome. • With primary adrenal tumors, ACTH should be suppressed (<5pg/ml). • With pituitary causes, it will be normal or slightly elevated (15-200pg/ml). • With ectopic ACTH secreting tumors, it will be markedly elevated.
Cushing Syndrome • High Dose Dexamethasone Test may be used to distinguish pituitary from non-pituitary causes of ACTH-dependent Cushing syndrome. • Rationale is that the high dose will notsuppress cortisol production from a primary adrenal neoplasm or ectopic ACTH secreting tumor.
Suspect Cushing Syndrome 24 hour urine free Cortisol X 3 days 100mg/24 hr. Cushing’s Syndrome Low dose Dexamethasone suppression test Equivocal (possible pseudo-Cushing’s) No suppression of plasma cortisol Suppresses Plasma cortisol (<5 ng/ml) Cushing’s Syndrome No cushing’s
Cushing’s Syndrome Late-afternoon/midnight measurement of plasma cortisol + ACTH Plasma cortisol >50 ng/ml, ACTH >50 pg/ml Plasma cortisol >50ng/ml Plasma ACTH <5 pg/ml No Cushing’s ACTH-dependant Cushings Syndrome ACTH-independent Cushing’s High dose dexamethasone suppression test ? Metyrapone stim. Test, ?inferior petrosal Sinus sampling Adrenal tumor or hyperplasia >50%reduction in cortisol <50% reduction in cortisol Pituitary tumor (Cushing’s disease) Ectopic ACTH Adrenal CT/MRI Pituitary CT/MRI Pituitary surgery Thoracic/abdominal CT/MRI Surgical removal Treatment of primary lesion Bilateral adrenalectomy Necessary occasionally cure Failure Pituitary irradiation or Bilateral adrenalectomy
Adrenal Insufficiency, Addisons Weight loss, anorexia 90% Nausea, vomiting 66% Weakness, tiredness, fatigue 94% GI complaints 61% abdominal pain 28% Diarrhea 18% Muscle pain 16% Salt craving 14% Hypotension, dizziness, syncope 14% Lethargy, disorientation 12%
Adrenal Insufficiency, Causes • Autoimmune • Steroid withdrawal • Adrenal atrophy (lymphocytic adenitis with fibrosis) • Malignant infiltration • Hemorrhage • Sepsis • Iatrogenic (post op) • Sarcoidosis, Tuberculosis
Adrenal Insufficiency, Diagnosis • Hyponatremia • Hyperkalemia • Azotemia • Hypercalcemia • 10-30% associated with other endocrine disorders • AM cortisol level, ACTH level • Rapid ACTH test • 0.25 mg IV cosyntropin • Measure cortisol before and 60 min after • Cortisol level should be >18mcg/dl at 60 min
Adrenal Insufficiency, Treatment • Acute – stress dose dexamethasone • Chronic – hydrocortisone (200-300mg) plus fludrocortisone (.05-1.0mg/day) • ACTH stim test to establish diagnosis
Hyperaldosteronism • Primary (suppressed renin) • Adrenal adenoma • Adrenal carcinoma • Bilateral hyperplasia • Secondary • Renal artery stenosis • Edematous states (cirrhosis, renal failure)
Hyperaldosteronism, Diagnosis • CT scan • Adrenal vein sampling • Urinary 18-hydroxycortisol – elevated in adenoma. • plasma hydroxycorticosterone (overnight recumbent)- > 100 in adenoma
Hyperaldosteronism, Diagnosis • Serum K < 3.6 mEq/L • Plasma renin activity (PRA) < 1 ng/ml • Plasma aldosterone >22 ng/dL • Urine aldosterone > 14 mcg/24hrs • Urine K > 40 mEq/24 hrs • Plasma aldosterone:PRA ratio > 50:1
Hyperaldosteronism, Treatment • Bilateral hyperplasia-medical, spironolactone, amiloride. • Unilateral adenoma- adrenalectomy.