Pharmacokinetics and Safety of Dexmedetomidine in Neonates Post Open Heart Surgery: Phase 1 Study
This Phase 1 trial evaluates the pharmacokinetics and safety of dexmedetomidine in neonates following open heart surgery. The study assesses individual and population pharmacokinetic parameters using advanced liquid chromatography and mass spectrometry. Secondary objectives include analyzing sedation levels, extubation readiness, and hemodynamic impacts. Preliminary results indicate that a continuous infusion of dexmedetomidine at 0.2 mcg/kg/hour is well-tolerated, showing promise for facilitating tracheal extubation in this vulnerable population.

Pharmacokinetics and Safety of Dexmedetomidine in Neonates Post Open Heart Surgery: Phase 1 Study
E N D
Presentation Transcript
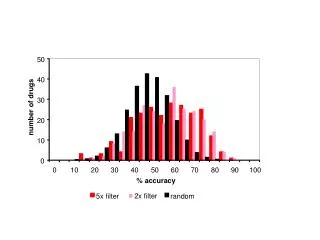
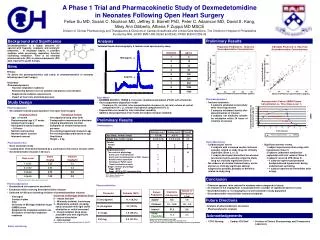
400 4 350 300 3 250 200 2 150 100 1 50 0 0 0 5 10 15 20 25 30 35 40 Time (hours) Plasma Concentration UMSS A Phase 1 Trial and Pharmacokinetic Study of Dexmedetomidine in Neonates Following Open Heart SurgeryFelice Su MD, Susan C. Nicolson MD, Jeffrey S. Barrett PhD, Peter C. Adamson MD, David S. Kang, Mary Ann Diliberto, Athena F Zuppa MD MSCE Division of Clinical Pharmacology and Therapeutics & Divisions of Cardiac Anesthesia and Critical Care Medicine, The Children’s Hospital of Philadelphia Funded by NIH, GCRC #M01-RR-00240 & NICHD, PPRU #HD037255-09 C. C. Preliminary Results Background and Significance Analysis Dexmedetomidine is a highly selective α2-agonist with hypnotic, analgesic and anxiolytic properties. In intubated adults, it provides sedation while preserving respiratory function facilitating extubation. There is no neonatal pharmacokinetic (PK) or pharmacodynamic (PD) data reported to guide therapy. Validated liquid chromatography & tandem mass spectrometry assay Population Predicted vs. Observed Dexmedetomidine Concentrations Individual Predicted vs. Observed Dexmedetomidine Concentrations 1500 pg/mL Aims Population Predicted Plasma Concentration (pg/mL) Primary • To define the pharmacokinetics and safety of dexmedetomidine in neonates following open heart surgery Secondary • Pharmacodynamics • Tracheal extubation readiness • Relationship between level of sedation and plasma concentration • Supplemental sedation requirements • Impact on heart rate and blood pressure Individual Predicted Plasma Concentration (pg/mL) 5 pg/mL Observed Plasma Concentrations (pg/mL) Observed Plasma Concentrations (pg/mL) • Base Model • NONMEM ADVAN 3, TRANS 4, first order conditional estimation (FOCE) with interaction • Two-compartment disposition model Clearance (CL, mL/min), inter-compartmental clearance (Q, mL/min) volume of central compartment (V1, L), volume of peripheral compartment (V2, L) • Exponential error model for inter-individual variability • Additive and proportional error model for random residual variability Pharmacodynamics • Tracheal extubation • 6 subjects extubated successfully while receiving infusion • 3 subjects extubated shortly after discontinuation of infusion • 5 subjects not medically suitable for extubation within 24 hours of initiation of infusion Study Design Representative Patient UMSS-Plasma Concentration vs. Time (Dose Level 1) Patient population • 36 evaluable neonates post-operative from open heart surgery Dexmedetomidine Plasma Concentration (pg/mL) UMSS Preliminary Results Demographics Pharmacokinetics • Dose escalation study • Loading dose immediately followed by a continuous intravenous infusion (CIVI) • Dexmedetomidine infusion ≤ 24 hours B. B. A. Conclusion * Preliminary results reflect dose level 1 and 2 Pharmacodynamics • Standardized intra-operative anesthetic • Extubation while receiving dexmedetomidine infusion • Collected for 48 hours following initiation of dexmedetomidine infusion: Pharmacokinetics • Clearance appears to be reduced in neonates when compared to infants • An infusion of 0.4 mcg/kg/hour is associated with a number of significant adverse events • Dexmedetomidine at 0.2 mcg/kg/hour is well-tolerated in study population • Dexmedetomidine may facilitate tracheal extubation Future Directions Acknowledgements 1Hospira, Precedex Product Label 2004 2Petroz GC, et al. Anesthesiology 2006. 105:1098–1110 3Su F, et al. The Children’s Hospital of Philadelphia. Data not yet published. Iselin-Chaves IA, et al. Anesth Analg 1998. 87: 949-55 Safety monitoring