Download
1 / 38
400 likes | 841 Vues
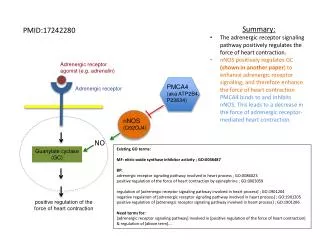
Dr. S. Parthasarathy MD., DA., DNB, MD ( Acu ), Dip. Diab.DCA, Dip. Software statistics- Ph d Mahatma Gandhi Medical college and research institute , puducherry , India. Adrenergic receptors . Ahlquist – 1948 . Progress . WHAT IS THIS ?? Two transmitters

E N D
Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab.DCA, Dip. Software statistics- Ph d Mahatma Gandhi Medical college and research institute , puducherry , India Adrenergic receptors
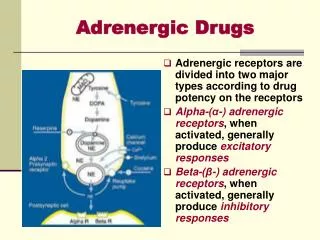
WHAT IS THIS ?? Two transmitters Adrenaline Acetyl choline Its noradrenaline Adrenergic receptors
α α 1 α 2 β β1 β2 β3 Classification
Dopamine DA 1 DA 2 Most of the drugs act on some other receptors also
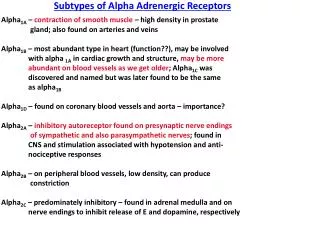
Vasoconstriction Metabolism Conscious status Nociception Alpha receptors
α 1 Smooth vessels of blood vessels Vasoconstriction Liver – glycogenolysis Intestine – contraction Alpha receptors
mydriasis (pupillary dilation due to contraction of the radial eye muscles), broncho constriction, uterine contracture, contraction of sphincters in the gastrointestinal and genitourinary tracts. α1-Stimulation also inhibits insulin secretion and lipolysis. α1-receptors that have slightly positive inotropic and negative chronotropic effects Alpha 1 agonists – minor
Platelet aggregation Sympathetic nerve endings Decrease norad release Pancreatic beta cell Decrease insulin release Alpha 2
Heart – force , rate, excitability increased Renal JG apparatus - ↑ rennin release Beta 1
Smooth muscle of bronchi, blood vessel, uterus bladder- vasodilation and relaxation Heart – force, rate increased Skeletal muscle – hypokalemia Beta cell pancreas- ↑ insulin Beta 2
Fat – thermogenesis Subcutaneous tissue Lipolysis Beta 3
Dopamine-1: vascular smooth muscle (renal, mesentery, coronary causing vasodilation),renal tubules (natriuresis, diuresis), juxtaglomerular cells (increased renin release). Dopamine-2: postganglionic sympathetic nerves (inhibits NE release), smooth muscle (renal, mesenteric causing possible constriction). Dopamine
Noradrenaline > adrenaline > > isoprenaline beta receptors Isoprenaline > adrenaline > noradrenaline Alpha receptors
After stoppage of beta blockers , there is sudden increase of beta receptors Pharmacological dynamism
Adrenergic agonists Dopamine Dopamine Phenyleph Clonidine Dobutamine Oxymetazoline Isoprenaline Noradrenaline Terbutalin norad Adrenaline Ephedrine Ephedrine
Adrenaline , noradrenaline and dopamine – Natural catecholamines Direct acting and indirect acting Differences
Alpha 1 Alpha 2 Beta 1 Beta 2 Summary
Anaphylaxis • alpha-adrenergic receptors, _____lessens the vasodilation and increased vascular permeability. action on beta- receptors, ________causes bronchial smooth muscle relaxation that helps alleviate bronchospasm, wheezing, and dyspnoea Adrenaline
Additives CPR Why we should use adrenaline
Direct B1 and B 2 and indirect alpha 1 May cause tachycardia and hypertension Ideal for spinal epidural hypotension especially in pregnant patients- should not cross placenta Ephedrine
Dobutamine Acts on b1 and b2, with minimal action on a1 receptors. It increases cardiac output and reduces afterload (b2effects on skeletal muscle). CardIogenic shock.
Vasodilation is predominant pathology Inotrope with minimal beta 2 action Use noradrenaline Sys, dias, MAP increase without CO increase No chronotropic effects Septic shock
Complete heart block, overdose of beta blocker or severe bradycardia unresponsive to atropine Acts on b1 and b2 receptors Isoprenaline Isoprenaline
Beta 1, alpha 1 and DA 1 and DA 2 Dopamine 2 µg / kg 5 µg / kg 10 µg / kg Cardiogenic shock with oliguria
Alpha and beta Inotropy with minimal vasodilation at low doses But alpha vasoconstriction predominates in higher doses Increases myocardial oxygen consumption – stress testing Use in patients where myocardial O2 consumption ?? Dobutamine
Sudden hypotension and aortic stenosis obstructive hypertrophic cardiomyopathy, Phenylephrine Nitrates and viagra induced BP fall
Dopamine and dobutamine individual or combination Vasopressin RV infarct – IV fluids and dobutamine Acute MI
Correction of the cause with dobutamine Adrenaline Isoprenaline where we need the highest kick and not bother about tachycardia Post cardiac surgery status
We want only beta 2 agonists Terbutaline and others Bronchial asthma
Adrenergic receptor agonist But hypotension Analgesia Sedation Alpha 2 agonist Clonidine
Preterm labour Beta 2 agonist Not much tachycardia not much hypotension Ritodrine , isoxsuprine
Adrenergic agonists Dopamine Dopamine Phenyleph Clonidine Dobutamine Oxymetazoline Isoprenaline Noradrenaline Terbutalin norad Adrenaline Ephedrine Ephedrine
Blockers labetolol labetolol Phent, phenoxy propranolol Butoxami Prazosin Yohimbine Aten Tamsulosin