Download
1 / 47
1.03k likes | 5.28k Vues
SIGNAL TRANSDUCTION BY ADRENERGIC AND CHOLINERGIC RECEPTORS. Andy Catling Ph.D. Department of Pharmacology Room 5238 acatli@lsuhsc.edu 568-4740. Adrenergic Receptors. Alpha Receptors: 1 : Contraction of vascular and genitourinary smooth muscle .

E N D
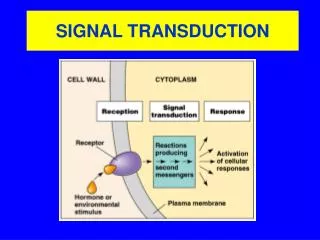
SIGNAL TRANSDUCTION BY ADRENERGIC AND CHOLINERGIC RECEPTORS Andy Catling Ph.D. Department of Pharmacology Room 5238 acatli@lsuhsc.edu 568-4740
Adrenergic Receptors • Alpha Receptors: • 1:Contraction of vascular and genitourinary smooth muscle. • 2:Contraction of vascular smooth muscle; decreased insulin secretion; aggregation of platelets; pre-synaptic inhibition of NE. • Beta Receptors: • 1: Positive inotropic and chronotropic effects on the heart. • 2: Relaxes vascular, bronchial, gastrointestinal and genitourinary smooth muscle; stimulates glyconenolysis and gluconeogenesis in the liver. • 3: Lipolysis in adipose tissue.
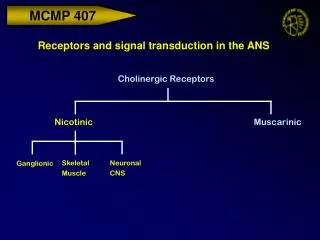
Cholinergic Receptors • Nicotinic Receptors: • NM (muscle): Depolarization of NMJ; Skeletal muscle contraction. • NN (neuronal): Activation of post ganglionic neurons. • Muscarinic Receptors: • M1: Depolarization of autonomic and CNS neurons • M2: Negative inotropic and chronotropic effects on the heart. • M3: Stimulates sweat, bronchial, salivary and gastric acid secretions; Increased NO production from vascular endothelium and vasorelaxation.
How does this work? • Different receptors can have reinforcing or opposing functions: e.g. 1 adrenergic receptors stimulate contraction of vascular smooth muscle whereas b2 adrenergic and muscarinic M3 receptors both cause relaxation. e.g. 1 adrenergic receptors stimulate contraction of heart muscle, whereas muscarinic M2 receptors inhibit myocardial contraction. Goal of these lectures: begin to understand the signal transduction mechanisms by which specificity is established. Note that this is still a work-in-progress: the human body is complex (!) and there are both gaps in our knowledge and exceptions to general rules
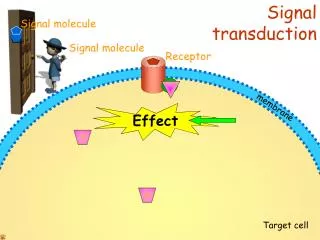
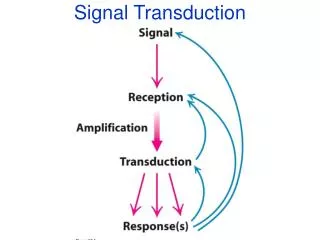
Components of Signal Transduction Signal transduction within cells is accomplished by combinations of: • 1st Messenger (extracellular signals e.g. epinephrine, acetylcholine) • Receptor • Effectors (e.g. adenylyl cyclase, phospholipases, kinases, ion channels etc) • 2nd messengers (cAMP, cGMP, inositol triphosphate, diacylgycerol, Ca2+ etc) • Downstream effectors required for specific functional outputs (e.g. muscle contraction, secretion)
How does this work? Specificity results from: • Differential expression and localization (junctionalvs extra junctional) of receptors • Different receptors couple to different signal transducers • Signal transducers/2nd messengers couple to different effectors in different tissues • Integration of reinforcing and antagonistic signals
b Adrenergic Receptors • b receptors differ in their location and sensitivity to Epinephrine and Norepinephrine (simplified!): b1 Myocardium E=NE b2 Smooth muscle E (essentially no affinity for NE) b3 Adipose tissue NE>E i.e. tissue response to agonist is governed by expression of receptor subtypes and ligand present • All threeb adrenergic receptors function through a major class of signal transducer: G-proteins • G-proteins couple b adrenergic receptors to adenylyl cyclase: b agonists increase intracellular cyclic AMP levels and protein kinase A activity, which in turn regulate downstream effectors
G-protein Activation-Deactivation Cycle GDP GDP + GTP Pi GDP GPCR* GTP + Effectors Effectors
Adrenergic Receptors • Beta Receptors • 1 Receptors • Gs (stimulatory): Activation of adenylyl cyclase and increased cAMP levels. • Positive inotropic and chronotropic effects on the heart; speeds conduction across the AV node. • Agonist: Dobutamine • Antagonist: Atenolol
b1 adrenergic receptors function through Gs to stimulate the effectoradenylylcyclaseto produce the 2nd messenger cyclic AMP • Activated Gs: • stimulates adenylyl cyclase to produce • cAMP • enhances activation of voltage gated Ca2+ • channels in the plasma membrane • cAMP: • activates protein kinase A, which directly • phosphorylates proteins (e.g. troponin I) • essential for cardiac muscle contraction • stimulates sodium/potassium influx which • opens voltage-gated Ca2+ channels • inhibits uptake of Ca2+ into cellular stores • cAMP hydrolyzed by phosphodiesterases Overall effect: increased intracellular Ca2+ concentration and phosphorylation of contractile proteins. Result: cardiac muscle cells expressing b1 receptors contract in response to epinephrine or norepinephrine.
Adrenergic Receptors • Beta Receptors • 2 Receptors • Gs: Activation of adenylyl cyclase and increased cAMP levels. • Relaxes vascular, bronchial, gastrointestinal and genitourinary smooth muscle, stimulates the uptake of potassium into skeletal muscle, stimulates glycogenolysis and gluconeogenesis in the liver. • Agonist: Terbutaline • Antagonist: Propranolol • Why does b1 stimulation cause contraction in cardiac muscle while b2 stimulation causes relaxation of smooth muscle – both elevate cAMP?
Different downstream effectors: different responses EPI, b1, cardiac muscle EPI, b2, smooth muscle protein kinase A Troponin I absent from smooth muscle. PKA phosphorylation of a different target, myosin light chain kinase, inhibits myosin function. Phosphorylation of contractile machinery proteins: e.g. Troponin I CONTRACTION RELAXATION
Different downstream effectors: different responses SMOOTH MUSCLE EPI, b2, Gs RELAXATION CONTRACTION
Adrenergic Receptors • Beta Receptors • 3 Receptors • Activate Gs protein, stimulates adenylate cyclase and increases cAMP levels. cAMP activates PKA which stimulates the lipase activity i.e. another context-specific effector • Adipose tissue: Lipolysis.
Adrenergic Receptors • Beta Receptors: summary • Receptors • b1, b2 and b3 ALL activate Gs which stimulates adenylyl cyclase and increases cAMP levels. • cAMP activates protein kinase A • Outcome depends on what PKA phosphorylates: e.g. Troponin in cardiac muscle (contraction); MLCK in smooth muscle (relaxation); lipase in adipose tissue
Adrenergic Receptors • Alpha Receptors: • 1:Contraction of vascular and genitourinary smooth muscle. • 2:Contraction of vascular smooth muscle but also indirect effects that lead to vasodilation. Also decreased insulin secretion, aggregation of platelets.
Adrenergic Receptors a1 and b2 receptors both signal through G-proteins, yet can cause opposite effects on the same tissue (e.g. genitourinary smooth muscle). How?
a1 and b2 signal through different G-proteins a Subunits aolf as a12 a13 at1 at2 agust ao1 ao2 ai1 ai3 ai2 az a15 a16 a11 aq a14 b1 b2 b4 b3 b5 g11 g1 gScone g10 g5 g12 g7 g2 g4 g3 gSolf b Subunits as Family a12 Family ai Family aq Family g Subunits
Adrenergic Receptors • 1 Receptors: • a1 receptors coupled to Gqnot Gs • Gq activates phospholipase C (PLC) causing production of inositol triphosphate (IP3) and diacyglycerol (DAG) from inositol phospholipids • Gq-linked receptor operated calcium channel • Overall effect is to increase intracellular calcium • Calcium-calmodulin stimulates myosin light chain kinase activity and hence contraction of vascular and genitourinary smooth muscle • Agonist: Phenylephrine • Antagonist: Prazosin
Epi, NE Interstitial fluid DAG PLC Gq 1 GTP GDP Contraction of vascular and genitourinary smooth muscle PIP2 IP3 Ca2+ IP3 IP3R Intracellular calcium pools
Different downstream 2nd messengers and effectors: different responses e.g. vascular or genitourinary smooth muscle EPI, a1, Gq EPI, b2, Gs RELAXATION CONTRACTION
IMPORTANT…..direction of response depends upon ligand concentration e.g. in vascular smooth muscle b2 a1 Gs, cAMP, VASODILATION a1 b2 LOW EPI b2 a1 Gq, Ca2+, overcomes cAMP effects, VASOCONSTRICTION HIGH EPI
Adrenergic Receptors a2 adrenergic receptors on vascular smooth muscle cause contraction How?
Adrenergic Receptors • direct effect on vascular smooth muscle is contraction mediated by extra-junctional2 receptors: • NE or Epi stimulation of a2 engages Gi/o classes of G-protein • Gi/o inhibits adenylyl cyclase thus decreasing cAMP levels • Gi/o increases Ca2+ influx • Decrease in cAMP allows calcium-calmodulin stimulation of MLCK activity, causing contraction
Gi and Gs have opposite effects on adenylylcyclase activity Epi, a2 adrenergic receptor
Direct effect of a2 on vascular smooth muscle: contraction Vascular smooth muscle Epi, a2 Gi CONTRACTION
Adrenergic Receptors BUT a2 adrenergic receptors also can cause vasodilationon How?
Indirect effect of a2 on vascular smooth muscle: relaxation and vasodilation Presynaptic Receptors (Autoreceptors)
Adrenergic Receptors • Pre-synaptic 2 receptors: indirectlycausevasodilation • stimulation of pre-synaptic a2 receptors by NE or EPI inhibits release of NE at the synapse • NE concentration in the adrenergic synapse is reduced decreasing stimulation of post-synaptic a1 receptors • Less post-synaptic a1/Gq activation, translates into less calcium-calmodulin stimulation of MLCK • Relaxation
Cholinergic Receptors • Muscarinic Receptors: • M1: Depolarization of autonomic and CNS neurons • M2: Negative inotropic and chronotropic effect on the heart. • M3: Smooth muscle contraction with ONE EXCEPTION: cause vascular smooth muscle relaxation and vasodilation; Glandular secretion Also M4 and M5. • Nicotinic Receptors: • NM (muscle): Depolarization of NMJ; Skeletal muscle contraction. • NN (neuronal): Activation of post ganglionic neurons.
Multiple acetylcholine-mediated effects: how? • Different subtypes of cholinergic receptors in different tissues.
Cholinergic Receptors • Muscarinic Receptors: • M1: Autonomic ganglia, CNS, some secretory glands. Cause depolarization of autonomic and CNS neurons • M2: Heart, CNS. Cause negative inotropic and chronotropic effects on the heart • M3: Smooth muscle; vascular endothelium and secretory glands. Cause smooth muscle contraction; glandular secretion; BUT also vasodilation i.e. as for adrenergic responses, tissue response is governed by expression of specific receptor subtypes
What accounts for the differences in Acetylcholine-mediated effects? • Different subtypes of cholinergic receptors in different tissues. • Different receptors are coupled to different G-proteins and hence different effectors.
Different muscarinic receptors couple to different G-proteins • Muscarinic Receptors: all G-protein linked • M1: Gq/11 Gastric secretion in parietal cells and depolarization of autonomic and CNS neurons • M2: Gi Negative inotropic and chronotropic effect on the heart. • M3: Gq/11 Stimulates smooth muscle contraction; sweat, bronchial and salivary secretions; paradoxical vasodilation.
Cholinergic Receptors • Muscarinic Receptors • M1 Receptors • Gq/11: Activation of phospholipase C generates DAG and IP3; IP3 increases intracellular calcium • i.e. M1 and a1 have similar signaling mechanism
Acetylcholine Interstitial fluid DAG PLC Gq M1 PKC GTP GDP Neurons: Depolarization of autonomic and CNS neurons PIP2 IP3 Ca2+ IP3 IP3R Intracellular calcium pools
Cholinergic Receptors • Muscarinic Receptors • M2 Receptors • Gi: inhibition of adenylyl cyclase and decreased cAMP • M2 and a2 have similar signaling mechanism • Reduced PKA phosphorylation of troponin I, negative inotropic and chronotropic effect on the heart (i.e. antagonistic to b1)
Cholinergic Receptors • Muscarinic Receptors • M3 Receptors • Gq/11: Activation of PLC, hydrolysis of IP3 and increased intracellular calcium, similar to M1. • Secretion (bronchial, sweat and salivary glands, gastric acid); contraction of most smooth muscle • Paradoxical relaxation of vascular smooth muscle and vasodilation: result of increased synthesis of NO and PGI2 in vascular endothelium
Indirect effect of M3 stimulation on vascular smooth muscle: vasodilation M3 Gq/11 Guanylyl cyclase COX – cyclo-oxygenase PCS – prostacyclinsynthase Gs Vasodilation Simplistically: the endothelial cell converts a Gq response (increased Ca2+) to a Gs response (increased cyclic AMP)
Cholinergic Receptors • Nicotinic Receptors: Cation Channels • NM: Depolarization of NMJ; Skeletal muscle contraction. • NN: Activation of post ganglionic neurons.
Cholinergic Receptors • Nicotinic Receptors: Cation Channel • NN Type • Autonomic ganglia: Activation of post ganglionic neurons in autonomic ganglia. • Agonist: Nicotine • Antagonist: Trimethaphan
K+ Na+ Ach Ach Ach Ach Binding K+ Na+ Open NN nicotinic receptors: Heteropentamers of and subunits or Homopentamers of subunits.
Cholinergic Receptors • Nicotinic Receptors: Cation channel • NM Type • Neuromuscular Junction: Depolarization of NMJ; Skeletal muscle contraction. • Heteropentamers of a, b, g and d subunits • Agonist: Acetylcholine • Antagonist: Tubocurarine