Understanding Systemic Lupus Erythematosus (SLE): Early Detection and Ocular Effects
Systemic Lupus Erythematosus (SLE) is a significant autoimmune disease particularly affecting young Black females who may present with a malar rash. Early detection is crucial for effective management and reducing the risk of complications like ocular toxicity from common treatments such as antimalarial agents (Aralen® and Plaquenil®). Key risk factors include female sex, increasing age, and family history. This lecture emphasizes the importance of comprehensive patient history and monitoring for ocular side effects, especially maculopathy, which can lead to irreversible damage if not identified early.

Understanding Systemic Lupus Erythematosus (SLE): Early Detection and Ocular Effects
E N D
Presentation Transcript
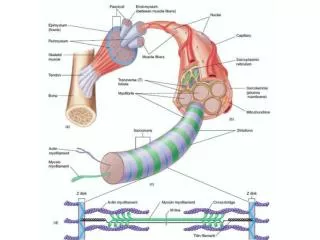
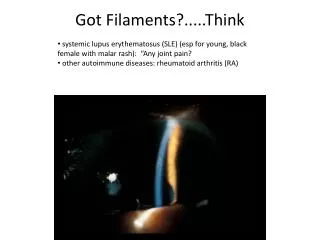
Got Filaments?.....Think • systemic lupus erythematosus (SLE) (esp for young, black female with malar rash): “Any joint pain? • other autoimmune diseases: rheumatoid arthritis (RA)
Reasons why auto immune disease is important to O.D.’s • 3rd most prevalent diseases after? • cancer • heart disease • Leading cause of death/disability in women • Ocular side effects of disease • Ocular side effects of medication used for treatment
Risk Factors for autoimmune disease • female sex • increasing age • overlap (10% with Type I DM have other autoimmune disease) • familial
O.D.’s concerns for autoimmune diseases • ocular side effects of autoimmune disease • ocular side effects of medications used to treat autoimmune disease • These points were emphasized at least 4 times during lecture!
Name the two antimalarial agents that are commonly used to treat autoimmune diseases. (in order of toxicity to the eye) • Aralen® (chloroquine) • > 250mg QD • Plaquenil® (hydroxychloroquine) • > 400 mg QD • Early detection ESSENTIAL;complete patient history crucial!
Describe early & later maculopathy from antimalarial agent usage: • Early • pigment stippling • mottling • loss of FLR • Later • Central granular hyperpigmentation with surrounding zones of depigmentation and hyperpigmentation • “Bulls-Eye” maculopathy • Usually bilateral
Differential diagnosis for maculopathy from antimalarial agents • Stargardt’s • dominant cone dystrophy • Resolved central serous chorioretinopathy (CSC) • ARMD
“For Boards” • “If it looks like a bulls eye, it probably is a bulls eye • Other clues: • Aralen® (chloroquine)/Plaquenil® (hydroxychloroquine) use above 250mg/400mg qd • Aralen® (chloroquine)/Plaquenil® (hydroxychloroquine) use for more than 10 years • bilateral presentation • Remember: • Once the macula looks like this, the dammage is permanent!
Reasons why maculopathy occurs from antimalaria agent usage • long half-lives of Aralen® (chloroquine) & Plaquenil® (hydroxychloroquine) • bind with RPE melanin • interference with RPE function • decreased photoreceptors, RPE migration
prognosis of retinal toxicity effects of antimalarial agents • excellent, if antimalarial agent halted early • “bull’s eye” pattern: irreversible and advanced dammage
“Take home” risk factors for maculopathy from antimalarial agents • Aralen® (chloroquine) dosage greater than 250 mg per day • Plaquenil® (hydroxychloroquine) dosage greater than 400 mg per day • more commonly used! • on medication (@ normal dosages) more than 10 years • patients with renal insufficiency taking smaller doses • Always ask if pt has kidney problems in history!
O.D. clinical management: antimalarialmaculopathy • Standard of Care: • Baseline Exam: good history including medications, dosages & duration of use • (red?) Amsler grid: monitor for paracentralscotoma • Humphrey 10-2 perimetry (possibly with red target) • retina exam with photography • Other items: • EOG • F-100 • FlAN • OCT
Follow-up care for antimalarialmaculopathy • if no problems • follow-up at 12 months • if reproducible scotoma or macular pigment changes • PCP notified of abnormal ocular findings • PCP and patient determine whether Rx change is indicated • follow-up at 3-6 months.
the most common condition for which Plaquenil® (hydroxychloroquine) is prescribed: • SLE: systemic lupus erythematosus • Others include: • rheumatoid arthritis (RA) • discoid lupus erythematosus • Sjogren’s syndrome • sarcoidosis
“For boards” • What is this a picture illustrating? • What other ocular condition might be associated with this? • chest xray of patient with sarcoidosis. • These patients may be taking Aralen® (chloroquine) or Plaquenil® (hydroxychloroquine). • Our biggest concern is retinal toxicity from the drugs • Other ocular signs may include chronic iritis.
other medications a patient with autoimmune disease may be on that can cause ocular side effects • (oral steroids) • higher risk of posterior subcapsular cataracts (PSCs) than topical • risk of elevating IOP (topical corticosteroids usually greater risk than oral)
Young African-American Female with Malar Rash?.....Think systemic lupus erythematosus (SLE)
“For Boards”—info about diagnosing systemic lupus erythematosus • classic autoimmune disease • anti-nuclear antibodies (ANAs) always present • ANA diagnostic testing is sensitive (for autoimmune disease), but it is not specificfor a particular disease. • Symptoms: chronic & variable • joints (#1 organ involved) • kidneys • skin • febrile
systemic lupus erythematosus (SLE) epidemiology: • young, black female adults • 1.4 million Americans • Also more common in Hispanic, Asian, and Native American women
Course of systemic lupus erythematosus: • variable & unpredictable • flare-ups & remissions over many years • can be fatal (15-20%); concomitant infections, renal failure, CNS disease • not curable; with early diagnosis and treatment, most lead healthy life • 20% are disabled
treatment of systemic lupus erythematosus: • treatment outlook increasingly favorable • antimalarials • Plaquenil® (hydroxychloroquine) • NSAIDs • corticosteroids • immunosuppressants
ophthalmic manifestations of systemic lupus erythmatosus: • keratoconjunctivitissicca (most common) • retinal involvement (parallels systemic course): cotton wool spots, hemorrhages • management: steroids, immunosuppressants, laser photocoagulation • episcleritis/scleritis • management: standard treatment with adequate systemic control • uveitis?
“Boards like for you to know” diagnostic points for thyroid disease • For Graves disease: • AI complexes mimic TSH. • Recall: Normally, T3 & T4 blood levels are monitored by hypothalamus & pituitary gland. As T3T4 go up, TRH & TSH levels go down, thyroid stimulation removed T3T4 production reduced, thus keeping T3T4 at a steady-state. • In Graves disease, autoimmune complexes mimic TSH, so blood T3T4 levels are elevated, while TRH and TSH hormones are lower than normal. The normal steady-state does not occur, and hyperthyroidism is the result.
What is ‘Uhthoff’s sign’, and what systemic disease is it associated with? • blurred vision when the body gets overheated from exercise, hot weather, fever, saunas, hot tubs, or any other source of heat • multiple sclerosis
ocular manifestations of multiple sclerosis • optic neuritis (retro bulbar) • “The doctor sees nothing (abnormal)” • but, “The patient sees nothing” • 75% of patients, up to 25% initially • Visual prognosis is good • usually returns
optometric management of multiple sclerosis • follow-up within a month, including visual field • every 3-6 months thereafter
autoimmune disease (after lupus) to know • rheumatoid arthritis • chronic • systemic • autoimmune • inflammatory • more serious; causes more eye side effects
rheumatoid arthritis vs. osteo arthritis • RA: • causes more systemic symptoms; patients are sicker • osteo patients’ symptoms are relieved with sleep; RA patent’s aren’t. • RA is generally symmetrical; osteo is not.
rheumatoid arthritis treatment (ophthalmic considerations) • Plaquenil® (hydroxychloroquine) • prednisone • (same ocular considerations as SLE therapy)
The “mackdaddy” of dry eye • Sjogren’s Syndrome • post menopausal women with dry eyes & sicca complex (dry mouth, nose, vagina) • can be primary (no collagen vascular disease) or secondary to other autoimmune disease • insidious • autoimmune lymphocyte /plasma cell infiltration/destruction of lacrimal and salivary glands. viral trigger, loss of testosterone
Sjogren’s syndrome treatment: • standard: • tears • ointments • punctal plugs or cautery • filamentary keratitis: • topical steroids • acetylcysteine (*know for boards*; Dr. Landgraf has never Rx’ed) • NaCl 5% • bandage soft CL • physical removal with forceps