Download
1 / 28
360 likes | 616 Vues
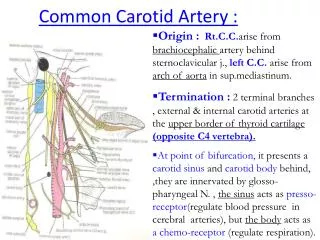
Eric Hager, MD Assistant Professor of Surgery Division of Vascular surgery University of Pittsburgh Medical Center. Natural History of Carotid Artery Disease. Cerebral Vascular Disease “Stroke”. 3 rd leading cause of death in the United States Incidence: 795,000 First stroke: 610,000

E N D
Eric Hager, MD Assistant Professor of Surgery Division of Vascular surgery University of Pittsburgh Medical Center Natural History of Carotid Artery Disease
Cerebral Vascular Disease“Stroke” • 3rd leading cause of death in the United States • Incidence: 795,000 • First stroke: 610,000 • Recurrent stroke: 185,000 • Annual US mortality: 136,000 • Morbidity • 15-30% permanently disabled • 20% require institutional care at 3 months Sources: Roger VL, et al. `American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics--2011 update: a report from the American Heart Association. Circulation. 2011 Feb 1;123(4):e18-e209. Epub 2010 Dec 15.
Cerebral Vascular Disease“Stroke” • Lifetime risk for stroke at 65 years of age • Men: 14.5% • Women: 16.1% • Economic • 2007 direct and indirect cost of stroke: $40.9 billion • Average lifetime cost of ischemic stroke: $140,048 Sources: Roger VL, et al. `American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics--2011 update: a report from the American Heart Association. Circulation. 2011 Feb 1;123(4):e18-e209. Epub 2010 Dec 15.
Stroke and Extracranial Carotid Artery Occlusive Disease Hemorrhagic: 13% Ischemic: 87% Source: Mackey WC. CHAPTER 92 – Cerebrovascular Disease : General Considerations. Rutherford’s Vascular Surgery. 7th Edition. 2010.
Extracranial carotid disease is associated with stroke • Symptomatic disease • Already experienced a neurologic event • High risk of recurrence • Secondary prevention • Asymptomatic disease • Incidentally found • Low, but significant, ongoing risk of an event • Primary prevention
MR and CT imaging: stroke extent and carotid stenosis Davis SM, Donnan GA. Secondary Prevention after Ischemic Stroke or Transient Ischemic Attack. N Engl J Med 2012;366:1914-22.
Cerebral vascular Occlusive Disease • Risk factors: • Male gender • Advancing age • Hypertension • Smoking • Diabetes • Atrial fibrillation • History of cerebrovascular disease
Natural History • What is the Natural History of carotid disease? • Asymptomatic? • Symptomatic? • * No contemporary studies • non-medically managed • best medical therapy (BMT)
Before BMT: Natural history of asymptomatic disease – severity of stenosis • 1986: 500 patients with asymptomatic carotid bruits and variable stenosis graded by ultrasound • Recorded TIA/Stroke rates • Study period 4 years (mean follow up 26 month) 19.5% 5.7% 2.1% Sources: Chambers BR. Norris JW. Outcome in patients with asymptomatic neck bruits. N Engl J Med. 1986;3 15:860-865
Before BMT: Natural history of asymptomatic disease - echogenicity • 1987: 296 patients evaluated • Stratified according to: • 1) Degree of stenosis by B-mode US • 2) Echogenicity of the carotid lesion • Gray-scale median >32 =dense • Gray-scale median <32 = echolucent • Evaluated neurologic events over a 3 year study period Sources: O’Holleran LW, Kennelly MM, McClurken M, Johnson JM. Natural history of asymptomatic carotid plaque. Am J Surg. 1987; 154:659-662
Before BMT: Natural history of asymptomatic disease - echogenicity • 1987: 296 patients evaluated • Stratified according to: • 1) Degree of stenosis by B-mode US • 2) Echogenicity of the carotid lesion • Gray-scale median >32 =dense • Gray-scale median <32 = echolucent • Evaluated neurologic events over a 3 year study period Support to the NEJM data – degree of stenosis correlates to neurologic event rates. Dense (calcified) plaque is less likely to cause TIA/strokes Sources: O’Holleran LW, Kennelly MM, McClurken M, Johnson JM. Natural history of asymptomatic carotid plaque. Am J Surg. 1987; 154:659-662
Before BMT: Natural history of asymptomatic disease – stenosis progression • 1984: Stroke - Roederer and colleagues examined 167 patients with <80% stenosis • Conclusion: Progressive disease leads to a higher risk of neurologic events Sources: Roederer GO, Langlois YE, Jager KA, Primozich JF, Beach KW, Phillips DJ, Strandness DE Jr. The natural history of carotid arterial disease in asymptomatic patients with cervical bruits. Stroke 1984;15: 605-613
Best Medical Therapy • Evolution of Best Medical Therapy (BMT) • Smoking cessation • Glycemic control • Anti-platelet (e.g., aspirin +/- dipyridamole, clopidogrel) • Lower hypertension (ACE, ARB, b-blocker) • Address dyslipidemia (statins)
ACST- asymptomaticendarterectomy v. medical therapy • Patients with >60% stenosis • 30 day results: • CEA: 2.5% • BMT: 0.7% • 5 year results: • CEA: 6.4% • BMT: 11.8% • P<0.0001 CEA Medical 0 1 2 3 4 5 Years after randomization Halliday A, Mansfield A, Marro J, Peto C, Peto R, Potter J, Thomas D; MRC Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group. Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet. 2004 May 8;363(9420):1491-502.
Natural history of untreated symptomatic disease • No randomized study is possible today in symptomatic disease • Consequently natural history is based on early observational studies
Natural history of symptomatic disease – ASA vs. Placebo Sources: 1) The Canadian Cooperative Study Group. A randomized trial of aspirin and sulfinpyrazone in threatened stroke. N Engl J Med 299: 53-59, 1978 2) Candelise L, Landi G, Perrone P, Bracchi M and Brambilla G. A randomized trial of aspirin and sulfinpyrazone in patients with TIA. Stroke. 1982;13:175-179 3) Fields WS, Lemak NA, Frankowski RF, Hardy RJ: Controlled trial of aspirin in cerebral ischemia. Stroke. 8:301-315 1977 324036 4)Bousser MG, Eschwege E, Haguenau M, et al.: “AICLA” controlled trial of aspirin and dipyridamole in secondary prevention of athero-thrombotic cerebral ischemia. Stroke. 14:5-14 1983 6401878
Natural history of symptomatic disease – ASA vs. Placebo Sources: 1) The Canadian Cooperative Study Group. A randomized trial of aspirin and sulfinpyrazone in threatened stroke. N Engl J Med 299: 53-59, 1978 2) Candelise L, Landi G, Perrone P, Bracchi M and Brambilla G. A randomized trial of aspirin and sulfinpyrazone in patients with TIA. Stroke. 1982;13:175-179 3) Fields WS, Lemak NA, Frankowski RF, Hardy RJ: Controlled trial of aspirin in cerebral ischemia. Stroke. 8:301-315 1977 324036 4)Bousser MG, Eschwege E, Haguenau M, et al.: “AICLA” controlled trial of aspirin and dipyridamole in secondary prevention of athero-thrombotic cerebral ischemia. Stroke. 14:5-14 1983 6401878
Natural history of symptomatic disease – ASA vs. Placebo In all trials there was a reduction of stroke rates with aspirin therapy. No further placebo trials have been conducted since. Sources: 1) The Canadian Cooperative Study Group. A randomized trial of aspirin and sulfinpyrazone in threatened stroke. N Engl J Med 299: 53-59, 1978 2) Candelise L, Landi G, Perrone P, Bracchi M and Brambilla G. A randomized trial of aspirin and sulfinpyrazone in patients with TIA. Stroke. 1982;13:175-179 3) Fields WS, Lemak NA, Frankowski RF, Hardy RJ: Controlled trial of aspirin in cerebral ischemia. Stroke. 8:301-315 1977 324036 4)Bousser MG, Eschwege E, Haguenau M, et al.: “AICLA” controlled trial of aspirin and dipyridamole in secondary prevention of athero-thrombotic cerebral ischemia. Stroke. 14:5-14 1983 6401878
North American Symptomatic Carotid Endarterectomy Trial • 1991- NASCET trial sought to compare outcomes of surgery vs. best medical management • 659 patients with symptomatic carotid disease • Stroke risk was directly related to degree of stenosis North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 1991 Aug 15;325(7):445-53.
North American Symptomatic Carotid Endarterectomy Trial • Stroke risk also correlated to number of risk factors: • Age >70 • SBP >160 • DBP>90 • Recent stroke • Stenosis >80% • Ulcerated plaque • Hx of tobacco use • Diabetes • Claudication • Hyperlipidema The study was stopped early due to the high stroke rates of medically managed patients. All patients recommended to have CEA North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 1991 Aug 15;325(7):445-53.
North American Symptomatic Carotid Endarterectomy Trial • 659 patients • 30 day results • CEA: 5.8% • BMT: 3.3% • 2 year results • CEA: 9% • BMT: 26% North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 1991 Aug 15;325(7):445-53.
Treatment of patients with asymptomatic disease • Best medical therapy (BMT) YES • High risk for open surgery? • Medical comorbidities • Difficult anatomy Patient with asymptomatic carotid stenosis ≥ 80% (>3 year life expectancy) NO • BMT + Open surgery (CEA)
Treatment of symptomatic patients • BMT + Stenting YES • High risk for open surgery? • Medical comorbidities • Difficult anatomy Patient with symptomatic carotid stenosis ≥ 60% NO • BMT + Endarterectomy
Conclusion: • The natural history of asymptomatic and symptomatic carotid disease is well understood • Asymptomatic patients, there is ongoing debate whether surgical intervention is ever warranted due to improved BMT • Most symptomatic carotid stenosis should undergo intervention