Download
1 / 1
10 likes | 136 Vues
Functional Neuroimaging of the Subjective Effects of Intranasal d-Amphetamine Kelly, T.H., Kluemper , C.T. , Emurian , C.E., Corbly , C.R., Martin, C.A., Andersen, A.H., Joseph, J.E., and Lile , J.A. University of Kentucky. Visual Analog Scale Ratings. Placebo 32 mg/70 kg. Placebo

E N D
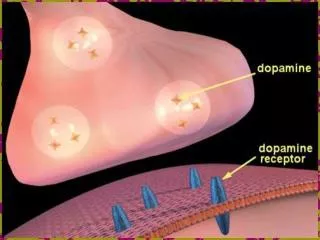
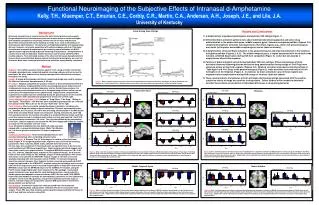
Functional Neuroimaging of the Subjective Effects of Intranasal d-Amphetamine Kelly, T.H., Kluemper, C.T., Emurian, C.E., Corbly, C.R., Martin, C.A., Andersen, A.H., Joseph, J.E., and Lile, J.A. University of Kentucky Visual Analog Scale Ratings Placebo 32 mg/70 kg Placebo 32 mg/70 kg Placebo 32 mg/70 kg Placebo 32 mg/70 kg Results and Conclusions 1) d-Amphetamine engendered prototypical stimulant-like VAS ratings (Figure 1). 2) Differential brain activation patterns were observed bilaterally following placebo and active drug administration in the paracentral gyrus, middle temporal gyrus, thalamus and globus pallidus (Figures 2-5). Unilateral hemispheric activation was observed in other brain regions [e.g., motor (left precentral gyrus) and visual (left superior and middle occipital gyrus) cortex (data not shown)]. 3) d-Amphetamine enhanced brain activation in the paracentral gyrus and reduced activation in the thalamus and globus pallidus (Figures 2, 4, 5). The middle temporal gyrus, a region associated with the default mode network, exhibited deactivation during VAS item completion (Figure 3). Active but not placebo d-amphetamine altered this response. 4) Patterns of brain activation varied during individual VAS item ratrings. Differential patterns of brain activation observed following placebo and active drug administration during ratings of ‘Feel Drug’ were observed across all four brain regions (Figures 2-5). Bilateral activation was observed during ratings of ‘Take Again’ and ‘Feel Drug’ in the paracentral gyrus (Figure 2), while activation occurred only in the left hemisphere of the thalamus (Figure 4). In contrast, no brain activation in any of these regions was engendered by d-amphetamine during VAS ratings of ‘Anxious’ (data not shown). 5) These results indicate that patterns of brain activation during drug ratings associated with the positive subjective effects of drugs are sensitive to drug effects. Future studies will be needed to determine whether these effects are predictive of individual differences in drug-taking behavior. Background Intranasal drug delivery is a useful method for both clinical practice and research. Drugs administered via the intranasal route have a faster onset of action and higher bioavailability compared to oral dosing, without the risk of injury and personal discomfort associated with routes requiring a needle stick, such as intravenous or intramuscular administration. The fast onset and high bioavailability of intranasal drug delivery, however, can also be associated with enhanced abuse potential. This study characterized intranasal d-amphetamine by examining neural activation via BOLD signals in brain regions during subjective reporting of drug effects. d-Amphetamine is a useful tool in human laboratory models because it can be safely administered to healthy subjects. Few controlled studies of the effects of intranasal d-amphetamine in humans have been published, despite reports that diverted prescriptions are used via this route. None have examined functional brain activation among healthy volunteers. Method Subjects: Six healthy Caucasian females, ages 20 to 27, using oral birth control that included a placebo phase, completed medical screening and gave written consent to participate. No other substance use history was reported or identified via urinalysis throughout the study. Design: A double-blind, placebo-controlled, randomized design was used to compare the effects of intranasal d-amphetamine (0, 32 mg). Procedure: Subjects completed one practice sessions to become familiarized with the magnetic resonance imaging facility and the neuroimaging process, behavioral and cardiovascular measures and daily laboratory routine. During these sessions, the subjects also practiced administration of an intranasal drug solution (saline), but no active doses of d-amphetamine were administered. Subjects then completed two experimental sessions that were scheduled during the placebo phase of the oral birth control regimen when estradiol and progesterone levels were at their nadir. Visual-Analog Rating Scales (VAS): Ratings of ‘Drug Effect,’‘Like Drug,’‘Willing to Take Again,’‘Stimulated,’ and‘Anxious’ were obtained by placing marks on a 100-unit line anchored with "Not at all" on the left and "Extremely" on the right. Daily Schedule: After successfully completing intake evaluations, including urine pregnancy and drug-use testing, subjects completed 15 minute assessments before (i.e., baseline, time 0) and 15, 30 and 45 min after drug administration in the MRI facility while brain activation (BOLD signal) was measured. During assessments, each VAS item was presented on 6 occasions according to a randomized block design such that each item was presented in a random order before any item was repeated. Each VAS item presentation consisted of a 30 s trial. The trial was initiated by the presentation of the item. Subject responses terminated the VAS item display and initiated a fixation crosshair for the remainder of the 30 s trial. Figure 1: Dose- and time-response function of intranasal d-amphetamine on ratings of Like Drug, Take Again, Feel Drug, Stimulated and Anxious on a Visual Analog Scale. Significant dose and/or dose x time interactions were observed on all but the anxious scales. Paracentral Gyrus Thalamus Left Hemisphere Right Hemisphere Left Hemisphere Right Hemisphere y = 48 y = 48 y = 48 Drug: Intranasal d-amphetamine was delivered using a syringe capped with a mucosal atomization device (Wolfe Tory Medical, Inc.). An active placebo consisted of 100 mg/mL magnesium sulfate. Cardiovascular Measures: Heart rate and blood pressure were recorded immediately after completing computer tasks. Brain Activation: A Siemens Trio 3.0 Tesla magnet is used to collect functional brain images. A T2*-weighted gradient echo sequence was used with the following parameters: 29ms echo time, 64x64 matrix, 224x224-mm field of view, 40 3.5-mm axial, slices acquired in interleaved order, 3s repetition time. A 3D shim was performed before all EPI image acquisitions. High-resolution structural images (with 1mm cubic voxels) were acquired with a T1-weighted MPRAGE sequence (TE = 2.93 ms, TR = 2100 ms, 256x256 matrix, acquired in the sagittal direction). An 8-channel head coil was used. Using the FSL package, images in each participant’s time series was motion corrected with the MCFLIRT module. Images in the time series were spatially smoothed with a 3D Gaussian kernel (FWHM = 7.5 mm) and temporally smoothed using a high-pass filter. Subjects’ motion corrected and smoothed 4D EPI image was registered to the ICBM152 T1 template using the registration matrix created from the three step process which involved registering the average EPI volume to the MPRAGE volume and the MPRAGE volume to the ICBM152 T1 template, using the FLIRT (Linear Image Registration Tool) module of the FSL package. Customized square waveforms were generated for each individual and were convolved with a double gamma hemodynamic response function (HRF) We then used FILM (FMRIB Improved Linear Model) to estimate the hemodynamic parameters for five explanatory variables; one for each VAS question, and generate statistical contrasts maps of interest. Contrast maps were warped into common MNI space before mixed-effect group analysis was performed. Data Analysis: Anatomical masks were then generated from the Automated Anatomical Labeling Atlas and parameter estimates (PE) were extracted for each subject. These PEs were then analyzed using repeated-measures ANOVA with dose (0 and 32 mg) and time as factors using SAS. x = 40 x = 40 Figure 4: Dose- and time-response function of intranasal d-amphetamine on parameter estimates of BOLD response during ratings of Take Again, Feel Drug and Like Drug in the left (left column) and Like Drug in the right (right column) thalamus (region indicated in the center panels). Significant dose and/or dose x time interactions were observed on all scales. Simple-effects tests indicated that significant differences between active and placebo doses were limited to sessions occurring post-dose administration. Figure 2: Dose- and time-response function of intranasal d-amphetamine on parameter estimates of BOLD response during ratings of Take Again, Feel Drug and Like Drug in the left (left column) and right (right column) paracentral gyrus (region indicated in the center panels). Significant dose and/or dose x time interactions were observed on all scales. Simple-effects tests indicated that significant differences between active and placebo doses were limited to sessions occurring post-dose administration. Middle Temporal Gyrus Globus Pallidus Right Hemisphere Left Hemisphere Right Hemisphere Left Hemisphere y = 48 z = 35 Figure 5: Dose- and time-response function of intranasal d-amphetamine on parameter estimates of BOLD response during ratings of Like Drug in the left (left column) and right (right column) globus pallidus (region indicated in the center panels). Significant dose and/or dose x time interactions were observed on the scale. Simple-effects tests indicated that significant differences between active and placebo doses were limited to sessions occurring post-dose administration. Figure 3: Dose- and time-response function of intranasal d-amphetamine on parameter estimates of BOLD response during ratings of Like Drug in the left (left column) and right (right column) middle temporal gyrus (region indicated in the center panels). Significant dose and/or dose x time interactions were observed on the scale. Simple-effects tests indicated that significant differences between active and placebo doses were limited to sessions occurring post-dose administration.