Gait disorders
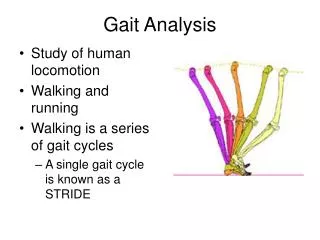
Gait disorders. Normal gait. The Gait cycle Comprised of swing and stance phases A stride is one full gait cycle Stance Starts with heel striking the ground and ends with pushing off via plantar flexion Swing Starts when toes lift off the ground and ends with the heel strike.

Gait disorders
E N D
Presentation Transcript
Normal gait • The Gait cycle • Comprised of swing and stance phases • A stride is one full gait cycle • Stance • Starts with heel striking the ground and ends with pushing off via plantar flexion • Swing • Starts when toes lift off the ground and ends with the heel strike
Examination of gait • Ensure patient’s legs are clearly visible • Ask the patient to walk normally for a few metres then back • Ask the patient to walk heel-to-toe (cerebellar lesion) • Ask the patient to walk on their heels (Foot drop caused by L4/5 lesion) • Ask the patient to walk on their toes (S1 lesion) • Romberg’s test – Ask patient to stand with feet together then close their eyes, compare the steadiness in both • Unsteadiness with eyes open shows cerebellar dysfunction • Unsteadiness after eye closure shows proprioceptive loss
Types of gait and their sources • Psychogenic or psychiatric – Variable • Cerebral – Cautious, Parkinsonian, ataxic, spastic, magnetic • Basal ganglia – Parkinsonism • Thalamus – ataxia • Cerebellum – ataxia • Brainstem – ataxia • Frontal lobe - apraxia • Spinal cord – spasticity or scissoring • Peripheral nerve (proprioception, vestibular, visual) – sensory ataxia, cautious • NMJ – waddling • Muscle - waddling
Causes of ataxia • Malabsorption syndromes leading to Vitamin E deficiency • Hypothyroidism • Aminoacidopatis, leukodystrophy • Alcohol • Lyme disease • Legionella • Sensory ataxia: posterior column spinal disorder (loss of proprioceptive sense), +ve Romberg’s, caused by diabetic neuropathy and Vit B12 deficiency
Cerebellar ataxia • Broad-based gait with posture erect but feet separated • Jerky, unsure steps varying in size • Patient staggers to affected side if there is a unilateral cerebellar lesion • Heel-to-toe walking is impaired • Turning can cause instability • Trouble starting a balance movement: rising off a chair or starting to stand up straight
Apraxic gait • Bilateral frontal lobe disease with the inability to plan and execute sequential movements • Wide-based, short strides, shuffling • Difficulty with beginning walking and turns • Strength is normal • Feet appear glued to the floor when erect but move normally when supine • Causes: vascular disease, communicating hydrocephalus
Hemiparetic gait • Residual sign of stroke • Abnormal posture of limbs produced by spasticity: leg swung in lateral arc Paraparetic gait • Caused by spinal cord disease or cerebral palsy • Both legs move in a slow and stiff manner with circular movements (scissoring gait)
Steppage gait • Due to foot drop (weakness of dorsiflexion) • Unilateral weakness: L5 radiculopathy, sciatic or peroneal neuropathy • Bilateral: distal polyneuropathy or lumbosacralpolyradiculopathy • Leg is lifted high above the ground to keep the toes high
Waddling gait • Caused by proximal limb weakness most often from myopathy, NMJ disease or proximal symmetric muscular atrophy • Trunk and pelvic muscle weakness results in excessive pelvic sway during movement (weakness of hip flexion)
Parkinsonian gait • Forward stoop, with modest flexion of hips and knees • Short rapid steps (shuffling gait) • Difficulty with gait initiation and turning • Upper body gradually leans further ahead of feet
Choreic gait • Intermittent irregular movement that disrupts smooth flow of normal gait (pelvic lurch)
Investigations • Imaging • MRI brain to see any cerebral lesions, normal pressure hydrocephalus, subdural haematoma, cerebellar atrophy, white matter disease • MRI spine to see spinals tenosis • Leg X-rays to see fractures • Lumbar puncture • Raised WCC or protein can indicate syhpillis infection (demyelination of nerves of the dorsal column) • Blood tests • Electrolytes: imbalances can impair motor function and gait • LFTs: sense of balance is particularly imapired in patients with chronic renal disease and those with hepatic failure • Toxic screen/drug levels • Testing for syphillis • BSL: diabetic neuropathy • Vit B12 – peripheral neuropathy
Treatment • Treat the cause • Cease drugs that worsen gait disorders • Muscarinic agonists • Anti-cholinesterases • Neuroleptics
Non-pharm treatment of gait disorders • Psychiatric counselling • Education • Physiotherapy • Modification of home to prevent falls • Canes: widen a person’s base of support • Crutches: increase the base of support and improve lateral stability and can be used for full weight bearing • Walking frame: improves balance by increasing patient’s base of support and enhancing lateral stability • Disadvantages • Difficulty manoeuvring through doorways and up stairs • Reduction in normal arm swing • Poor posture with abnormal flexion of the back
Consequences and complications • Falls • Injuries sustained in a fall are a major cause of morbidity and a major reason for hospital admission • Physical disability • Social impact: restriction of daily functioning, loss of independence, decreased quality of life