LIVER, GALLBLADDER, PANCREAS
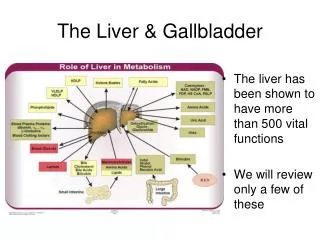
LIVER, GALLBLADDER, PANCREAS. Liver Jaundice Hepatitis Cirrhosis Tumors Gallbladder Pancreas. LIVER ANATOMY. Central area. Portal area. LIVER MICROSCOPIC. Duct. Vein. Artery. HEPATIC INJURY. Degeneration or accumulation Necrosis Inflammation Regeneration Fibrosis.

LIVER, GALLBLADDER, PANCREAS
E N D
Presentation Transcript
LIVER, GALLBLADDER, PANCREAS • Liver • Jaundice • Hepatitis • Cirrhosis • Tumors • Gallbladder • Pancreas
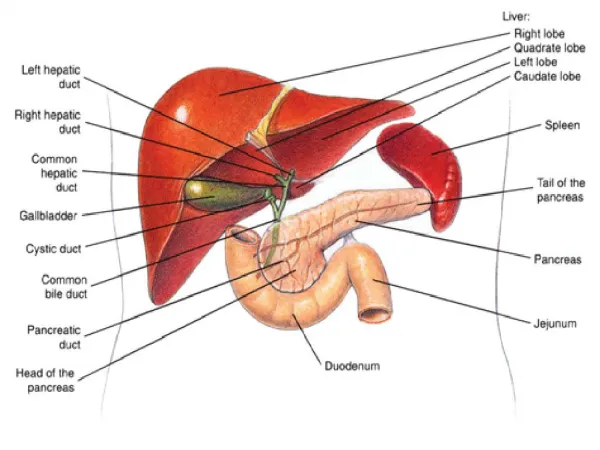
LIVER ANATOMY Central area Portal area
LIVER MICROSCOPIC Duct Vein Artery
HEPATIC INJURY • Degeneration or accumulation • Necrosis • Inflammation • Regeneration • Fibrosis
JAUNDICE • Excess bilirubin >2-3 mg/dl • Bilirubin metabolism • Unconjugated • Conjugated
JAUNDICE • Increase bilirubin production • Decreased hepatic uptake • Impaired conjugation • Impaired hepatic excretion • Cholestasis • Intrahepatic: cell injury • Extrahepatic: duct obstruction
VIRAL HEPATITIS • Hepatitis A • Hepatitis B • Hepatitis C • Hepatitis D • Hepatitis E • Hepatitis G • EBV, CMV, Herpes
HEPATITIS A • Common • RNA virus • Fecal or oral transmission • Incubation 15-45 days • No carrier or chronic disease
HEPATITIS B • DNA virus • Parenteral / sexual spread • Incubation 30-180 days • Serology • Carrier, chronic, cirrhosis • Risk malignancy • Vaccine
HEPATITIS C • RNA virus • Incubation 7-8 weeks • Parenteral, sexual spread • Carrier, chronic, cirrhosis • Risk malignancy • No vaccine
OTHER HEPATITIS VIRUSES • Hepatitis D • RNA virus • Associated with hepatitis B • Hepatitis E • Rare in the U.S. • RNA virus • Waterborne? • Hepatitis G (RNA similar to C) • ? Prevalence and significance • WHAT’S NEXT?????
ACUTE VIRAL HEPATITIS • Resolution in 8 weeks • Symptoms • Histology • Panlobular disarray • Inflammation • Hepatocyte necrosis • Fulminant: massive necrosis • Can become chronic
CHRONIC HEPATITIS • Abnormal liver function for >6 weeks • No longer use terms chronic active or chronic persistent • Grade activity and stage • Determine etiology
CIRRHOSIS • Cirrhosis • Diffuse • Fibrosis • Regeneration hepatocytes • Etiology • Fatty liver disease 60-70% • Viral 10%
CIRRHOSIS • Others • Biliary diseases • Metabolic/ genetic • Cryptogenic
CIRRHOSIS H&E Trichrome
CIRRHOSIS • Nonspecific symptoms • Liver failure • Portal hypertension • Ascites • Collateral venous channels • Splenomegaly • Neoplasm
CIRRHOSIS Esophageal varix Ascites
CIRRHOSIS- Fatty Liver Disease • ETOH Pathogenesis • Toxin • Nutritional deprivation • Other • Obesity • DM • Medications
HEMOCHROMATOSIS • Iron: liver, pancreas, heart + • Genetic • Homozygous recessive • Chromosome 6 • Secondary overload
HEMOCHROMATOSIS • Morphology • Hemosideron • Fibrosis • Treatment • Phlebotomy
WILSON’S DISEASE • Accumulation of copper; liver, brain, eyes • Autosomal rec • Morphology • Acute / chronic • Steatosis • Necrosis • Cirrhosis • Chelation D-Penicillamine
HEPATIC TUMORS • Benign and malignant • Cysts • Bile ducts • Blood vessel • Hepatocyte • Metastases
BILE DUCT NEOPLASMS • Bile duct adenoma • Gray nodule incidental finding • Bland proliferation ducts • Bile duct carcinoma • Thorotrast, liver fluke • Poor prognosis, late detection
HEPATOCELLULAR ADENOMA • Benign • Association with oral contraceptives • Presentation • Acute abdomen • Intra-abdominal bleed • Histology: bland hepatocytes and no bile ducts
HEPATOCELLULAR CARCINOMA- HEPATOMA • Malignant • Most common primary adults • Aflatoxin, cirrhosis, Hep B & C • Serum alpha-fetaprotein • Histology • Atypical hepatocytes • More than 2-3 cell plates • Poor prognosis
METASTATIC TUMORS • Often multiple nodules • Any primary- GI, lung, breast • CEA may be elevated if metastatic colon • Histology of primary tumor
BILIARY SYSTEMANATOMY • Gallbladder • Fundus • Body • Neck • 60-70% common orifice with pancreatic duct
BILIARY SYSTEMANATOMY • Microscopic- no mm or submucosa • Mucosa • Fibromuscular layer • Subserosal fat • Serosa • Physiology • Concentration • Delivery
CHOLELITHIASIS • Common- 10-20% of adults • Most gallstones silent • Association with inflamed gallbladder • Complications
CHOLELITHIASIS - STONE FORMATION • Pathogenesis • Supersaturation • Initiation • Growth • Types • Cholesterol (85% radiolucent) • Bilirubin (50-75% radiopaque)
CHOLELITHIASISRISK FACTORS • Cholesterol stones • Ethnicity • Age / sex • Diet / drugs • Pigment stones • Chronic hemolysis • Cirrhosis • Biliary infection
CHOLELITHIASISCOMPLICATIONS • Obstruction • Biliary colic • Cholecystitis • Gallstone illeus • May predispose to cancer?
CHOLECYSTITIS • 4th- 6th decade, F > M • Acute • Severe RUQ pain • Chemical, bacterial, reflux • Neutrophils, gangrene? • Chronic • Vague symptoms • Stones (90%) • Fibrosis, chronic inflammation • Acalculous
TUMORSGALLBLADDER • Carcinoma • 5th among GI malignancies • Peak incidence in 7th decade • Whites > blacks, F > M • 65-90% associated stones • Adenocarcinoma, poor survival
PANCREASANATOMY Exocrine – acini and ducts Endocrine - islets
ETIOLOGYACUTE PANCREATITIS • Cholelithiasis • Alcoholism • Trauma • Drugs • Septisemia, infection • Metabolic: hyper – Ca++ and lipids • Idiopathic