Trans-catheter Aortic Valve Replacement: a UK update.
290 likes | 553 Vues
Trans-catheter Aortic Valve Replacement: a UK update. Dr Martyn Thomas Guys and St Thomas’ Hospital. So, is there a clinical need for less invasive method of replacing the aortic valve??. Severe Symptomatic Aortic Stenosis is a fatal condition.

Trans-catheter Aortic Valve Replacement: a UK update.
E N D
Presentation Transcript
Trans-catheter Aortic Valve Replacement: a UK update. Dr Martyn Thomas Guys and St Thomas’ Hospital
So, is there a clinical need for less invasive method of replacing the aortic valve??
Severe Symptomatic AorticStenosis is a fatal condition. “Surgical intervention should be performed promptly once even… minor symptoms occur”1 Valvular Aortic Stenosis in Adults(Average Course) Chart: Ross J Jr, Braunwald E. Aortic stenosis. Circulation 1968;38 (Suppl 1) 1 C.M. Otto. Valve Disease: Timing of Aortic Valve Surgery. Heart 2000 Chart:: Ross J Jr, Braunwald E. Aortic stenosis. Circulation. 1968;38 (Suppl 1):61-7.
31.8% did not undergo intervention, most frequently because of comorbidities
Prof. Alain CribierFirst Clinical Experiences First described percutaneous aortic valve interventions in 1985 Proved that a stent could be deployed without removing the diseased native valve Implanted first percutaneous aortic valve on a patient on April 16, 2002
Currently available systems in the UK. • Corevalve: trans-femoral • Registry complete. CE mark. Now in commercial phase. • Edwards Sapien Valve: trans-femoral and transapical. • European Registry complete at the end of Jan. CE mark for both approaches. Now in commercial phase.
Self-Expanding Multi-level Support Frame • Diamond cell configuration • Nitinol (memory shaped) • Multi-level design incorporates three different areas of radial and hoop strength • Low radial force areaorients the system • Constrained area toavoid coronariesand featuringsupra-annularvalveleaflets • High radial forcefor secure anchoring – no recoil – constant force mitigates leak • Radiopaque
Porcine Pericardial Tissue Valve • Specifically designed for transcatheter delivery • Single layer porcine pericardium • Tri-leaflet configuration • Tissue valve sutured to frame • Standard tissue fixation techniques • 200M cycle AWT testing completed • Supra-annular valvefunction • Intra-annular implantationand sealing skirt
18F Delivery Catheter System Over-the-wire 0.035 compatible 12F shaft body 18F distal end Dual speed releasehandle
Technology Progress & Total Experience Generation 1 25F Transcatheter 14 patients Generation 2 21F Transcatheter 2004-2005 Generation 3 18F Percutaneous 65 patients* 2005-2006 184 patients** * Including 2 ReDo ** Updated August 30, 2007 Including Expanded Evaluation Registry Oct 2006
CoreValve PAVR ReValving™ System Updated August 31, 2007
Procedural Results – N=175 Procedural Success161 (92%) Mean Total Procedure Time 170 ± 77 Minutes Mean ReValving™ Time 11 ± 14 Minutes Discharged with CoreValve 159 (91%) Discharged after surgical conversion 3 (2%)
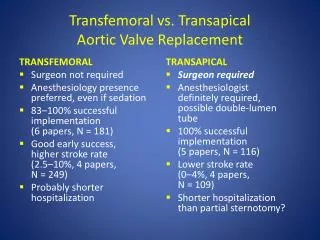
Edwards SAPIEN™ THV Access to the aortic valve Transapical Approach Transfemoral Approach
Cribier-Edwards™ and Edwards SAPIEN™ THV* Aortic Transfemoral/Transapical Trial Implants (21 Dec 07 Update) * The Edwards SAPIEN™ valve incorporates bovine pericardial tissue and TFX™ treatment
RetroFlex RetroFlex II RetroFlex II Offers: • Greatly improved native valve crossability • Smoother tracking • Improved handle functionality • Fewer system components
The UK position • 15 centres would like to start a programme. • Active centres, n=6. • Number of cases: • - Corevalve 71 • - Edwards 16 • Early Mortality approx 7%. 3/87 cath lab deaths, 5/87 in patient deaths (2 non cardiac) and 6/87 deaths at 3/12. • Also pacemaker, surgical conversion, peripheral vascular complications, stroke, pericardial drain. • Complex procedure but considering the patient mix encouraging.
Training • Centre selection currently controlled by industry. • Responsible attitude being taken. • MHRA (or whatever they are now called!) happy and do not feel central control is necessary. • Training consists (in general) of theory, simulators, observation and cases performed with proctors. • 2008 an interesting, dangerous and challenging year!!
UK Funding • Currently undergoing a NICE assessment. • Most centres trying to use a “surgical” tariff. • “Top ups” being locally negotiated with PCTs. • Early “NICE” assessment (like PFO closure) may facilitate the process.
Trans-catheter Aortic Valve Replacement: a UK update.Conclusions • 2008 will be an exciting but “dangerous” year for trans-catheter heart valve replacement. • Training and case selection is all. • Irresponsible use of the device could set Europe and the UK back for many years. • This exciting development in interventional cardiology could well be the future for tertiary/surgical centre intervention (at least in the medium term!)