Download
1 / 18
210 likes | 568 Vues
Common? fUndus and Choroidal Dystrophies. Spring? 2008 Optometry 8370. Introduction. Readings Kanski, Chapter 18, pp.690-692 Alexander, Chapter 7. F & C Dystrophies. Things To Think About….. F & C disease in the genes Inherited retinal diseases < 200,000 in the US

E N D
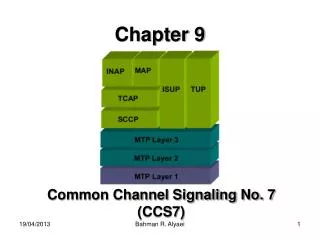
Common? fUndus and Choroidal Dystrophies Spring? 2008 Optometry 8370
Introduction • Readings • Kanski, Chapter 18, pp.690-692 • Alexander, Chapter 7
F & C Dystrophies • Things To Think About….. • F & C disease in the genes • Inherited retinal diseases < 200,000 in the US • Is not “rare if it is in your chair” • My approach to these conditions
F & C dystrophies • Things To Think About….. • Conditions are associated with Symmetry • Think hereditary if OU, not ? • Management and electrodiagnostics • No cure for any of these conditions • Research into genetic causes • May bring effective and lasting treatments
Retinitis Pigmentosa (RP) • Introduction • Most common of the hereditary retinal dystrophies and degenerations • Group of inherited retinal diseases • Affecting the photoreceptors • myopes • Symptoms • Nyctalopia (night vision loss) • Visual field constriction
rp • Signs (first seen) • Attenuated arterioles • “Bone spicule” pigmentation • along the veins in mid periphery and anterior • RPE changes • Also (later in course) • Cystoid macular edema (CME) • Disc drusen • Posterior subcapsular cataract • Pale waxy disc • Vitreal syneresis and pigment
RP • Retinal Course • Mid-peripherythen anterior and posterior • Inverse RP: central VA affected first • Text: rod-cone>cone-rod variants • Typical patient • Childhood night blindness • Late 20’s: VF sxs • Severe vision problems: 40’s • Minimal functional vision: 60’s
RP • Other forms • Retinitis sine pigmento • Retinitis punctata albescens: retinal white “dots” • Sector RP
RP • Besides sxs and signs…..what helps with the Diagnosis? • Full visual field • To monitor progression • Early ring scotoma • Then constriction”tunnel vision” • Central 10 degree VF to monitor • ERG (electroretinography) • May monitor progression • If reduced or delayed at the start • If flat at the start, monitor with? • Like what with glaucoma testing? Wake Up!
RP • Electrodiagnostics: ERG • Measures the electrical response of the eye to a flash of light • For rod/cone disorders • Dilation, electrodes (earlobe, forehead, contact lens) • Can be scotopic or photopic • Waveform is generated: a-b amplitude reduced in RP
RP • Diagnosis • ERG (electroretinography) • Aids with differential diagnosis • Vasculitis, pigmented paravenous retinochoroidal atrophy: phenotypically similar • Congenital stationary night blindness • Similar sxs • Normal a-wave (photoreceptors) • Reduced b-wave (Mueller and bipolar cells) or electronegative wave
RP • Genetics • About 50% of cases • No family history • No associated syndrome • The other 50% • 40% are AD or AR • 10% are sex-linked recessive • ADRP: sxs later in life • ARRP or XRP: sxs in teen years • Quicker progression vs ADRP • You may be asking, why do I need to know this data?
RP • Genetics • Testing available for family members and to confirm diagnosis if needed • Mutations in RHO (rhodopsin) • Mutations in peripherin/RDS gene • For example
RP • And Associated Syndromes (NBEO) • Usher Syndrome • moderate to severe hearing impairment • Birth or soon thereafter • Progressive vision loss from RP • 10,000-15,000 Americans • Types • I: early balance and hearing deficits, RP in early adolescence • II: moderate to severe hearing impairment, normal balance, RP in later adolescencs • III:eventual hearing problems and RP • A number of Usher genes identified
RP • Other syndromes (both very rare) • Laurence-Moon: hypogonadism, RP, mental retardation (MR), spastic paraplegia (lower body muscle disease) • Bardet-Biedl: autosomal recessive, MR, obesity, delayed sexual development, RP, kidney problems
RP • Management • As we speak, no FDA-approved medical treatment to cure or slow progression • Daily supplement of 15,000 IU or Vitamin A in palmitate form may slow progression in adults • Low Vision Aids • Clinical Trials and Investigational Studies • Retinal transplantation • Neurotrophic factors for cell rescue • Vaccinations against neurodegeneration • Gene replacement therapy • Interference RNA (to stop genetic mutations)
RP • Management • Once Diagnosis Is Made: • Signs, sxs, VF, ERG, genetic testing? • Counseling • Vitamin A (avoid vitamin E) • Low Vison referral if needed • Genetic counseling / generating a pedigree • Monitor every 6-12 months: VF, DFE, fundus photography, driving issues • Treatment of CME, cataracts if present