Snake bites
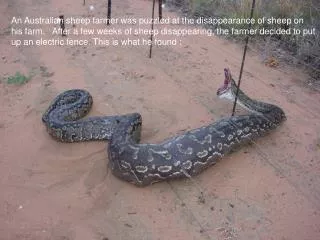
Snake bites. Hussein Unwala Dr. Ingrid Vicas February 4, 2010. Objectives. Identifying Venomous Snakes Signs of Envenomation Treatment of Presumed Snakebites. Identifying the Pit Viper. Prairie rattlesnake - coiled and rattling Longest fangs 3-4 cm Significant local tissue destruction.

Snake bites
E N D
Presentation Transcript
Snake bites Hussein Unwala Dr. Ingrid Vicas February 4, 2010
Objectives • Identifying Venomous Snakes • Signs of Envenomation • Treatment of Presumed Snakebites
Prairie rattlesnake - coiled and rattlingLongest fangs 3-4 cmSignificant local tissue destruction
“Red on Yellow Kills a Fellow” Hey Doc! Is This Snake Poisonous? Identifying Coral Snakes Sonoran Coral Snake
Hey Doc! Is This Snake Poisonous? “Red on Black, Venom Lack” Milk Snake - nonvenomous
Is the patient Envenomated? • Characteristics of a Venomous Snakebite • # strikes • Depth of envenomation • Size of snake • Potency/amount of venom injected • Size/health of victim • Location of bite
So how does this venom work? • “mosaic of antigens” • Proteolytic enzymes, procoagulants/anticoagulants, cardiotoxins, hemotoxins, neurotoxins • Venom is both circulating and tissue-fixed • Thus, anti-venom can halt progression, but won’t reverse clinical findings
What Clinical Signs are Present? • Local Reactions
What Clinical Signs are Present? • Systemic Signs • Venom travels via lymph/superficial veins to enter circulation • Mild: weakness, malaise, nausea, restlessness • More Severe: confusion, abdominal pain/V/D, tachycardia, hypotension, blurred vision, salivation, metallic taste in mouth • Rare: DIC, MODS • In some envenomations, neurotoxins predominate • Anaphylaxis
What Lab Findings might you expect? • Platelets 10-50,000 • Fibrinogen approaches Zero • PT, PTT immeasurably high • The majority of patients have no clinical bleeding!
Okay, now what? • Observing asymptomatic patients • 8-12 hours, if skin broken, and unable to ID snake • Pressure immobilization? • Do not occlude venous+arterial flow! • Broad, firm, constrictive wrap at 50-70mmHg • NOT recommended for NA pit viper envenomations • Venom Removal? • No benefit of negative pressure venom extraction
Okay, now what? • Delineate extent of edema, measure diameter of extremity • Look for any signs of clinical bleeding • Labs initially, then q 4-6 h • Tetanus • Analgesia/Anxiolysis
What About Antivenom? • First line therapy for moderate-severe envenomations • CroFab : ovine-derived Fab fragment • Fewer hypersensitivity reactions vs equine derived • Infused IV in 4-6 vials reconstituted in NS • Initiated at slow rate; if no signs of anaphylactoidrx, then rate is increased to complete the infusion over 1 hour • If progressive limb swelling, thrombocytopenia, coagulopathy, dose repeated prn • Once symptoms controlled, maintenance doses of 2 vials q 6h x 3 doses
Surgery? • Initial routine use of tissue excision, fasciotomy, or “exploration and debridement” not recommended • Surgical debridement usually done 3-6 days post envenomation
Other Management Points Low rates (0-3%) of wound infections No rationale for routine use of corticosteroids or anthistamines Careful followup of patients who received CroFab recurrence phenomenon serum sickness, delayed type hypersensitivity Fetal loss may be as high as 43% for bites during pregnancy Avoid any activity where risk of bleeding increased!!
What about exotic snakes? • Efforts should be made to identify snake • Once snake identified, antivenom should be obtained • Local zoos, poison centers, snake collector • Give antivenom if signs of envenomation (ie fang marks!) • Compression immobillization of entire extremity