Download
1 / 45
490 likes | 597 Vues
Learn about Trypanosoma parasites causing African trypanosomiasis, their life cycle, geographic distribution, and impact on humans and animals in Africa. Dr. Adnan S. Jaran provides a comprehensive overview of these mastigophora protozoa.

E N D
BLOOD AND TISSUE PROTOZOA MASTIGOPHORA Blood Flagellates
TRYPANOSOMA Dr. Adnan S Jaran
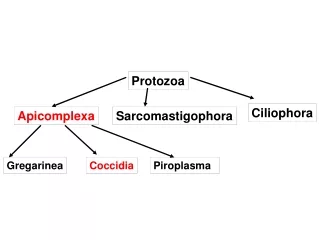
Classification • Trypanosomes are a group of kinetoplastid protozoa distinguished by having only a single flagellum. • All members are exclusively parasitic, found primarily in insects. • A few genera have life-cycles involving a secondary host, which may be a vertebrate or a plant. • These include several species that cause major diseases in humans. Dr. Adnan S Jaran
History The condition has been present in Africa since at least the 14th century, and probably for thousands of years before that. The causative agent and vector were not identified until 1902–1903 bySir David Bruce, and the differentiation between protozoa was not made until 1910. The first effective treatment, Atoxyl, anarsenicbased drug developed byPaul EhrlichandKiyoshi Shigawas introduced in 1910 but blindness was a serious side effect. Dr. Adnan S Jaran
Trypanosoma brucei is a parasitic protist species that causes African trypanosomiasis (or sleeping sickness) in humans and nagana in animals in Africa. There are 3 sub-species of T. brucei; T. b. brucei, T. b. gambiense and T. b. rhodesiense. Dr. Adnan S Jaran
These obligate parasites have two hosts - an insectvector and mammalian host. Because of the large difference between these hosts the trypanosome undergoes complex changes during its life cycle to facilitate its survival in the insect gut and the mammalian bloodstream. It also features a unique and notable variable surface glycoprotein (VSG) coat in order to avoid the host's immune system Dr. Adnan S Jaran
The insect vector for T. brucei is the tsetse fly (Glossina spp ). The parasite lives in the midgut of the fly (procyclic form), until it migrates to the salivary glands for injection to the mammalian host on binding. The parasite lives within the bloodstream (bloodstream form) where it can reinfect the fly vector after biting. Dr. Adnan S Jaran
Later during a T. brucei infection the parasite may migrate to other areas of the host. A T. brucei infection may be transferred human to human via bodily fluid exchange, primarily blood transfer. Dr. Adnan S Jaran
There are three different sub-species of T. brucei, which cause different variants of trypanosomiasis. T. brucei gambiense - Causes slow onset chronic trypanosomiasis in humans. Most common in central and western Africa, where humans are thought to be the primary reservoir T. brucei rhodesiense - Causes fast onset acute trypanosomiasis in humans. Most common in southern and eastern Africa, where game animals and livestock are thought to be the primary reservoir Dr. Adnan S Jaran
T. brucei brucei - Causes animal African trypanosomiasis, along with several other species of trypanosoma. T. b. brucei is not human infective due to its susceptibility to lysis by human apolipoprotein L1 However, as it shares many features with T. b. gambiense and T. b. rhodesiense (such as antigenic variation) it is used as a model for human infections in laboratory and animal studies. Dr. Adnan S Jaran
Geographic distribution and epidemiology The disease is found in two forms, depending on the parasite, either Trypanosoma brucei gambiense or Trypanosoma brucei rhodesiense. T. b. gambiense is found in central and western Africa; it causes a chronic condition that can extend in a passive phase for months or years before symptoms emerge. T. b. rhodesiense, is the acute form of the disease but has a much more limited range. It is found in southern and eastern Africa; its infection emerges in a few weeks and is more virulent and faster developing. Dr. Adnan S Jaran
The disease has been recorded as occurring in 36 countries, all in sub-Saharan Africa. It is endemic in southeast Uganda and western Kenya and kills more than 40,000 Africans a year. Humans are the main reservoir for Trypanosoma brucei gambiense, but this species can also be found in pigs and other animals. Wild game animals and cattle are the main reservoir of T. b. rhodesiense. Dr. Adnan S Jaran
African Trypanosomes. • African trypanosome – protozoan - causes fatal neurologic disease – trypanosomiasis. • Trypanosoma brucei rhodesiense & Trypanosoma brucei gambiense– Human sleeping sickness. • Trypanosoma brucei nagana (N’gana) in cattle. • Geographic distribution limited to sub-Saharan Africa by tsetse fly vector.
Life cycle The tsetse fly is large, brown and stealthy. While taking blood from a mammalian host, an infected tsetse fly (genus Glossina) injects metacyclic trypomastigotes into skin tissue. The parasites enter the lymphatic system and pass into the bloodstream (1). Inside the host, they transform into bloodstream trypomastigotes (2), are carried to other sites throughout the body, reach other blood fluids (e.g., lymph, spinal fluid), and continue the replication by binary fission(3). The entire life cycle of African Trypanosomes is represented by extracellular stages. A tsetse fly becomes infected with bloodstream trypomastigotes when taking a blood meal on an infected mammalian host (4,5). In the fly's midgut, the parasites transform into procyclic trypomastigotes, multiply by binary fission (6), leave the midgut, and transform into epimastigotes (7). The epimastigotes reach the fly's salivary glands and continue multiplication by binary fission (8). The cycle in the fly takes approximately 3 weeks to progress. Dr. Adnan S Jaran
Trypanosoma b. gambiense &T. b. rhodesienseLife cycle Dr. Adnan S Jaran
Trypanosoma b.gambiense &T.b.rhodesiense Thin blood film containing Trypomastigote stage: • “S” shape • Have small Kinetoplast near blunted, posterior end . • Conspicuous undulating membrane with flagellum. • One nucleus • This is Dividing stage in definitive host. ------------------------------------------------ • Infective stage: Trypomastigote Disease: African trypanosomiasis or sleeping sickness. Vector: Glossina spp. ( Tsetse fly) Drug of choice: Melarsoprol, Suramin, Pentamidine, Eflornithin. Dr. Adnan S Jaran
Trypanosoma cruzi Dr. Adnan S Jaran
Trypanosoma cruzi Thin blood film containing Trypomastigote stage: Size range: 12-35 um long by 2-4 um wide. • Shape: “C” or ”U” in stained blood films. • Appearance: Long and slender • Nucleus: One, located anterior to the kinetoplast. • Large Kinetoplast near the pointed posterior end. • Inconspicuous undulating membrane. ----------------------------------------------- • Infective stage: Trypomastigote • Vector:Triatoma spp. (Triatomid bug). • Disease: American Trypanosomiasis ( chagas’ disease). Dr. Adnan S Jaran
Trypanosoma cruziis found in many countries in the Americas, and is carried by insects to animals and human in much the same way as its African counterpart, although rather than the tsetse fly, the vecters are bedbugs or "assassin" flies. Trypanosoma cruziwas once thought to be confined to Brazil and its surrounding area, but recently cases of Chagas' disease have been reported as far north as southern North America. Immigrants from Central America and Mexico are thought to be the cause of the disease's migration northward. Dr. Adnan S Jaran
Trypanosoma cruzi life cycle Dr. Adnan S Jaran
Trypanosoma cruzi Amastigotes in stained rat skeletal muscle section: Intracellular Amastigotes. • Size range: 3 by 5 um. • Shape: Round to oval • Nucleus: One, usually off center. • Other feature: Present Kinetoplast This is the dividing stage in host. ----------------------------------------------- • Infective stage: Trypomastigote • Vector:Triatoma spp. ( Triatomid bug). • Disease: American Trypanosomiasis (chagas’ disease). Dr. Adnan S Jaran
Trypanosoma cruzi • Epimastigotes in culture: Size range: 9-15 um Appearance: Long and slightly wider than promastigote form. Nucleus: One, located in posterior end. Other features: Kinetoplast located anterior to the nucleus. Undulating membrane: Extending to the half of body length. Free flagellum, extending from anterior end. Dr. Adnan S Jaran
Clinical features Symptoms begin with fever, headaches, and joint pains As the parasites enter through both the blood and lymph systems, lymph nodes often swell up to tremendous sizes Winterbottom's sign, the telltale swollen lymph nodes along the back of the neck may appear If untreated, the disease slowly overcomes the defenses of the infected person, and symptoms spread to include anemia, endocrine, cardiac, and kidney diseases and disorders The disease then enters a neurological phase when the parasite passes through the blood-brain barrier. Dr. Adnan S Jaran
The symptoms of the second phase give the disease its name; besides confusion and reduced coordination, the sleep cycle is disturbed with bouts of fatigue punctuated with manic periods progressing to daytime slumber and nighttime insomnia. Without treatment, the disease is invariably fatal, with progressive mental deterioration leading to coma and death. Damage caused in the neurological phase can be irreversible. Dr. Adnan S Jaran
In addition to the bite of the tsetse fly, the disease is contractible in the following ways: • Mother to child infection: the trypanosome can cross the placenta and infect the fetus, causing prenatal death. • Laboratories: accidental infections, for example, through the handling of blood of an infected person and organ transplantation, although this is uncommon. • Blood transfusion Dr. Adnan S Jaran
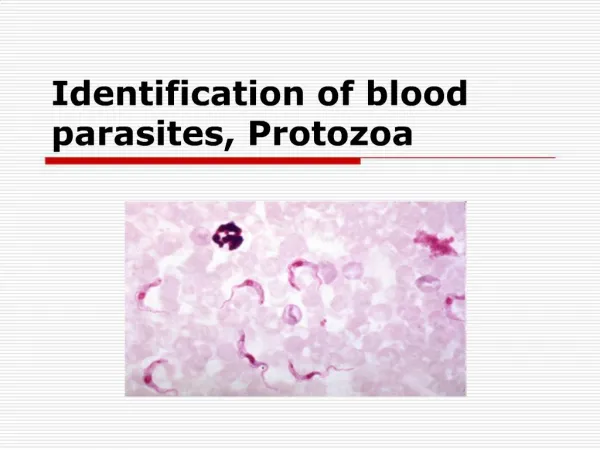
Laboratory diagnosis • The diagnosis rests upon demonstrating trypanosomes by microscopic examination of chancre fluid, lymph node aspirates, blood, bone marrow, or, in the late stages of infection, cerebrospinal fluid. • A wet preparation should be examined for the motile trypanosomes, and in addition a smear should be fixed, stained with Giemsa (or Field), and examined. • Concentration techniques can be used prior to microscopic examination. For blood samples, these include centrifugation followed by examination of the buffy coat; Dr. Adnan S Jaran
Treatment The current standard treatment for first stage disease is: • Intravenous pentamidine (for T.b. gambiense); or • Intravenous suramin (for T.b. rhodesiense) The drug Eflornithine— previously used only as an alternative treatment for sleeping sickness due to its labour-intensive administration — was found to be safe and effective as a first-line treatment for the disease in 2008, according to the Science and Development Network's Sub-Saharan Africa news updates. Dr. Adnan S Jaran
Leishmania Dr. Adnan S Jaran
Leishmaniaare protozoa belonging to the order Kinetoplastida and the family Trypanosomatidae. They are dimorphic parasites which present as two principal morphological stages : the intracellular amastigote, within the mononuclear phagocytic system of the mammalian host, and the flagellated promastigote within the intestinal tract of the insect vector and in culture medium. • The amastigote stage is a round or oval body about 2-6 µm in diameter, containing a nucleus, a kinetoplast and an internal flagellum seen clearly in electron micrographs. The amastigotes multiply within the parasitophorous vacuoles of macrophages.The promastigote stage has a long and slender body (about 15-30 µm by 2-3 µm), with a central nucleus, a kinetoplast and a long free anterior flagellum. Dr. Adnan S Jaran
Leishmania sp. • Leishmania tropica ( causes cutaneous leishmaniasis ). • Leishmania braziliensis ( causes muco-cutaneous leishmaniasis). • Leishmania donovani ( causes visceral leishmaniasis) Dr. Adnan S Jaran
History Leishmaniasis is a disease caused by protozoanparasites that belong to the genus Leishmania and is transmitted by the bite of certain species of sand fly, including flies in the genus Lutzomyia in the New World and Phlebotomus in the Old World. The disease was named in 1901 after the ScottishpathologistWilliam Boog Leishman and Donovan in India. This disease is also known as Leichmaniosis, Leishmaniose, leishmaniose, and formerly, Orient Boils, Baghdad Boil, kala azar, black fever, sandfly disease, Dum-Dum fever or espundia. Dr. Adnan S Jaran
Life cycle • Leishmaniasis is transmitted by the bite of female phlebotomine sandflies. The sandflies inject the infective stage, metacyclic promastigotes, during blood meals. (1)Metacyclicthat reach the puncture wound are phagocytized by macrophages(2)and transform intoamastigotes. (3)Amastigotes multiply in infected cells and affect different tissues, depending in part on whichLeishmaniaspecies is involved. (4)These differing tissue specificities cause the differing clinical manifestations of the various forms of leishmaniasis. Sandflies become infected during blood meals on an infected host when they ingest macrophages infected with amastigotes. (5,6)In the sandfly's midgut, the parasites differentiate into promastigotes, (7)which multiply, differentiate into metacyclic promastigotes and migrate to the proboscis(8). Dr. Adnan S Jaran
Life cycle Dr. Adnan S Jaran
Leishmania sp. Dr. Adnan S Jaran
Leishmania tropicaPromastigotes Promastigote in culture: Size range: 9-15 um Appearance: Long and slender. Nucleus: One, located in or near center. Other features: Kinetoplast, located in anterior end. Single free flagellum, extending from anterior end. ----------------------------------------------- Infective stage: Promastigote Diagnostic stage: Amastigote culture from skin lesion.Immunological techniques. Disease: Cutaneous Leishmaniasis (Also known as Old World leishmaniasis, Oriental sore,and Baghdad or Delhi boil). Vector: Phlebotomus spp. (Sandfly) Dr. Adnan S Jaran
Leishmania braziliensisPromastigote • Skin ulcer smear(Amastigotes): • Size range: 3 by 5 um. • Shape: Round to oval • Nucleus: One, usually off center. • Other feature: Present Kinetoplast ----------------------------------------------- Infective stage: Promastigote. Diagnostic stage: Amastigotes in stained Biopsy of the infected ulcer Disease: Mucocutaneous leishmaniasis Or espundia Vector: Lutzomyia spp. (sandfly). Dr. Adnan S Jaran
Leishmania donovaniAmastigotes Bone Marrow aspirate Showing Amastigotes: • Size range: 3 by 5 um. • Shape: Round to oval • Nucleus: One, usually off center. • Other feature: Present Kinetoplast. --------------------------------------------- Infective stage: Promastigote. Diagnostic stage: Amastigotes in stained aspirate of the infected bone marrow. Disease: Visceral leishmaniasis Or kala azar Vector: Phlebotomus spp. (sandfly). Dr. Adnan S Jaran
Signs and symptoms The symptoms of leishmaniasis are skin sores which erupt weeks to months after the person affected is bitten by sand flies. Other consequences, which can become manifest anywhere from a few months to years after infection, include fever, damage to the spleen and liver, and anaemia. Dr. Adnan S Jaran
Visceral leishmaniasis - the most serious form and potentially fatal if untreated. • Cutaneous leishmaniasis - the most common form which causes a sore at the bite site, which heal in a few months to a year, leaving an unpleasant looking scar. This form can progress to any of the other three forms. • Diffuse cutaneous leishmaniasis - this form produces widespread skin lesions which resemble leprosy and is particularly difficult to treat. • Mucocutaneous leishmaniasis- commences with skin ulcers which spread causing tissue damage to (particularly) nose and mouth. Dr. Adnan S Jaran
Cutaneous leishmaniasis ulcer on left forearm Dr. Adnan S Jaran
Diagnosis Leishmaniasis is diagnosed in the haematology laboratory by direct visualization of the amastigotes(Leishman-Donovan bodies). Buffy-coat preparations of peripheral blood or aspirates from marrow, spleen, lymph nodes or skin lesions should be spread on a slide to make a thin smear, and stained with leishman's or Giemsa's stain (pH 7.2) for 20 minutes. Amastigotes are seen with monocytes or, less commonly in neutrophil in peripheral blood and in macrophages in aspirates. They are small, round bodies 2-4um in diameter with indistinct cytoplasm, a nucleus and a small rod shaped kinetoplast. Occasionally amastigotes may be seen lying free between cells. Dr. Adnan S Jaran
Treatment There are two common therapies containing antimony (known as pentavalent antimonials), meglumine antimoniate (Glucantime) and sodium stibogluconate (Pentostam). It is not completely understood how these drugs act against the parasite; they may disrupt its energy production. Dr. Adnan S Jaran