Download
1 / 1
20 likes | 315 Vues
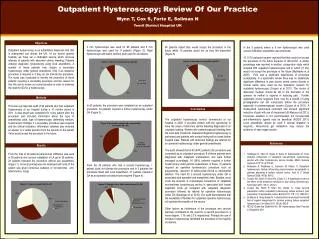
Outpatient Hysteroscopy; Review Of Our Practice Wynn T, Cox S, Forte E, Soliman N Yeovil District Hospital UK. Objectives. 3 mm hysteroscope was used for 85 patients and 5 mm hysteroscope was used for 9 patients (Figure 2). Rigid hysteroscope and saline medium were used for all patients. .

E N D
Outpatient Hysteroscopy; Review Of Our Practice Wynn T, Cox S, Forte E, Soliman N Yeovil District Hospital UK Objectives 3 mm hysteroscope was used for 85 patients and 5 mm hysteroscope was used for 9 patients (Figure 2). Rigid hysteroscope and saline medium were used for all patients. Outpatient hysteroscopy is an established diagnostic test that is widespread use across the UK. At our district general hospital, we have set a dedicated service which receives referrals of patients with abnormal uterine bleeding. Patients undergo diagnostic hysteroscopy using local anaesthetic. A number of these patients may require a secondary hysteroscopy under general anaesthetic (GA) if an operative procedure is required or if they do not tolerate the procedure. The study was conducted to identify the proportion of those patients requiring a secondary procedure and the reason for this. We aim to review our current practice in order to minimise the need for GA for a hysteroscopy. 84 patients stated they would accept the procedure in the future whilst 10 patients would not as they felt discomfort (Figure 5) In the 9 patients where a 5 mm hysteroscope was used cervical infiltration anaesthetic was employed. 10 (11%) patients however reported that they would not accept the procedure in the future because of discomfort. A similar percentage was reported in another prospective study which included 283 outpatient hysteroscopies and in which (11.3%) would not accept the procedure in the future (Mcllwaine et al 2009). Pain was a significant determinant of procedure acceptability. In a systematic review there was no statistically significant difference in pain scores where carbon dioxide or normal saline were used as the distension medium for outpatient hysteroscopy (Cooper et al 2011). The choice of distension medium should be left to the discretion of the operator as neither is superior in reducing pain . Further systematic review suggests there may be a benefit of using prostaglandins but not misoprostol before the procedure especially in postmenopausal women (Cooper et al 2011). A double-blind randomised controlled trial showed significant reduction of pain with use of misoprostol (El-Mazny et al 2011). Conscious sedation is not recommended, but non-steroidal anti-inflammatory agents may be beneficial (RCOG 2011). Local anaesthetic should be used if cervical dilatation is required). Intracervical gel installation may reduce the incidence of vaso-vagal reaction. Methods This was a prospective audit of 94 patients who had outpatient hysteroscopy at our hospital during a 10 months period in 2011. A data sheet was completed for every patient after the procedure and included information about the type of anaesthesia used, type of hysteroscope, distending medium, hysteroscopic findings, if a secondary procedure was required and the clinical indication. Information obtained also included an answer to a verbal question from the operator to the patient if she would accept the procedure in the future. In 60 patients, the procedure was completed as an outpatient procedure. 34 patients required a further hysteroscopy under GA (Figure 3). Conclusions The outpatient hysteroscopy service commenced at our hospital in 2000. It provides women with the opportunity to have the cause of abnormal uterine bleeding diagnosed in an outpatient setting. Women with postmenopausal bleeding form the main bulk of patients. Outpatient diagnostic hysteroscopy is performed and patients with normal finding will not need further hospital visits. Patients with abnormal findings are referred for an operative hysteroscopy under general anaesthesia. The audit showed that in 60 (64%) patients the procedure was completed as an outpatient procedure. 8 of these patients were diagnosed with malignant endometrium and were further managed accordingly. 34 (36%) patients required a further hysteroscopy under general anaesthesia; of these, 31 patients required an operative hysteroscopic procedure such as polypectomy, resection of submucosal fibroid or endometrial ablation. The need for a second hysteroscopy under GA is associated with operative and anaesthetic risks. Besides, more costs are incurred. A cost-analysis comparison of outpatient see-and-treat hysteroscopy service is associated with lowest treatment costs as compared with outpatient diagnostic procedure followed by referral for operative hysteroscopy under GA (Saridogan et al 2010). Our audit demonstrates that the availability of facilities for outpatient operative hysteroscopy will optimise the benefits of the service. Other factors as intolerance of the procedure and cervical stenosis contributed to the need for a second procedure to a minor degree; 1.1% and 2.1% respectively. Perhaps the use of miniature hysteroscope facilitated the procedure in the majority of patients. References Results From the total of 94 patients paracervical infiltration was used in 38 patients and cervical installation of LA gel in 28 patients. 28 patients tolerated the procedure without any anaesthetic (Figure 1). Cervical priming was not employed and none of the patient was given conscious sedation or non-steroidal anti-inflammatory drugs. • Saridogan E, Tiden D, Sykes D, Davis N, Subramanian D. Cost-analysis comparison of outpatient see-and-treat hysteroscopy service with other hysteroscopy service models. Minim Invasive Gynecol 2010’17 (4):518-25 • Mcllwaine K, Readman E, Cameron M, Maher, P. Outpatient hysteroscopy: factors influencing post-procedure acceptability in patients attending a tertiary referral centre. Aust N Z ObstetGynecol 2009, 49 (6): 650-2 • Cooper NA, Smith P, Khan KS, Clarke TJ. A systematic review of the effect of the distension medium on pain during hysteroscopy. FertilSteril 2011, 95 (1): 264-71 • Cooper NA, Smith P, Khan KS, Clarke TJ. Does cervical preparation before outpatient hysteroscopy reduce women’s pain experience? A systematic review. BJOG 2011, 118 (11): 1292-301 • El-Mazny A, Abou-Salem N. A double-blind randomized controlled trial of vaginal misoprostol for cervical priming before outpatient hysteroscopy. FertSteril 2011, 96 (4): 962-5 • RCOG Green-top Guideline No: 59. Hysteroscopy Best Practice in Outpatient 2011. From the 34 patients who had a second hysteroscopy, 1 patient could not tolerate the procedure and in 2 patients the procedure failed with local anaesthetic. 31 patients needed a GA as an operative procedure was required (Figure 4).