Download
1 / 11
120 likes | 428 Vues
Dive into a comprehensive case study of a 55-year-old female with chronic panuveitis presenting corneal melt, detailing her treatment journey from infection to immunosuppressive therapy and corneal transplant.

E N D
Pathology Case Presentation Corneal Melt Jeremy B. Wingard, MD
Case History • 55 year old female with longstanding history of panuveitis OS. • Past medical history includes Lupus and Sjogren’s syndrome. • She is maintained on systemic methotrexate and prednisone, as well as ocular prednisolone and intermittent periorbital steroids during flares.
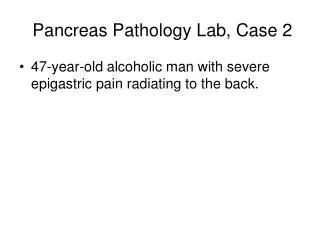
Acute Presentation • Patient developed increasing pain and decreased vision in the two days following a subtenon’s Kenalog injection. • Exam in ER: Corneal ulcer OS (three distinct infiltrates) with inferior corneal thinning. • Treated as inpatient for infectious keratitis (cultures positive for group A Streptococcus). Eventually cornea perforated and was glued twice.
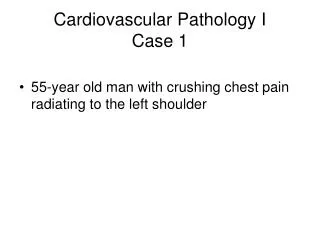
After second gluing Glue filling perforated cornea Infiltrate Edge of contact lens Hypopyon
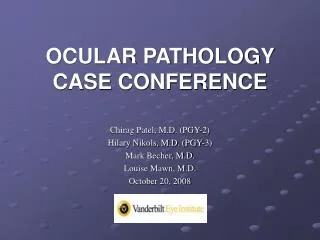
Further course • Immune melt of the cornea continued, with persistent hypopyon, infiltrates, and thinning. • Course reversed after patient received several doses of Remicade (Infliximab, monoclonal antibody against human TNFα). • At this point a scar developed, and the eye was quiet. Corneal transplant was undertaken.
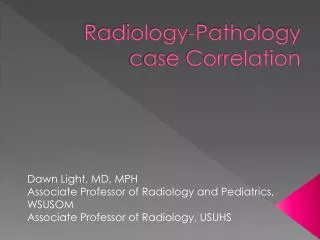
Post-transplant Host tissue Clear corneal graft
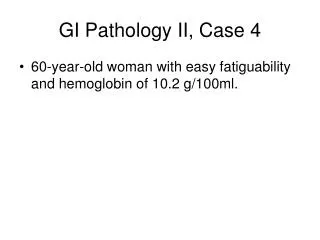
Mixed acute and chronic inflammation Lymphocytes Neutrophil
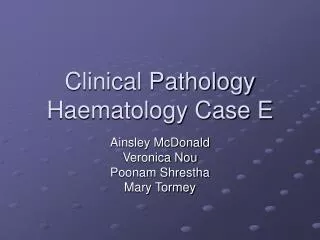
Corneal ulcer/thinning Full thickness cornea Disorganized epithelium Endothelium lost in processing Thinning Stromal scarring Stromal pigment
Discussion • Autoimmune inflammatory disease presents a great difficulty clinically when the course involves infection. • Although it is imperative to control inflammation, all anti-inflammatory therapies are inherently pro-infectious and so must be delayed. • In this case, the patient had a proven bacterial infection, but her response to infection, with corneal melt, was far beyond the normal response. • Clinical practice is to treat infection aggressively initially, then start anti-inflammatory therapy.
Corneal Stromal Pigment Differential • Iris pigment – post-perforation with iris prolapse, likely in this case. • Corneal tattoo – rule out by history • Corneal blood staining – possible to induce hyphema with surgery, although not noted clinically in this case • Metallic foreign body – sometimes found despite negative history
Diagnosis CHRONIC PANUVEITIS COMPLICATED BY INFECTIOUS AND IMMUNE-MEDIATED KERATITIS AND CORNEAL MELT.