Central Nervous System by DR IMTIAZ
520 likes | 699 Vues
Pathology. Central Nervous System by DR IMTIAZ. NEURON. Principal functional unit of CNS Neurons —incapable of cell division:

Central Nervous System by DR IMTIAZ
E N D
Presentation Transcript
Pathology Central Nervous Systemby DR IMTIAZ
NEURON • Principal functional unit of CNS • Neurons —incapable of cell division: • Specialized system of auto-regulation of cerebral blood flow, metabolic substrate requirements, the absence of conventional lymphatic system, a special CSF circulation, limited immunologic surveillance • These render nervous system vulnerable to unique pathological processes and reactions to injury differing from other systems of body
GLIA • Neuroectodermal origin: Macroglia • Astrocytes • Oligodendrocytes • Ependymal cells • Choroid lining cells • Bone marrow derivation: Microglia • Neuropil
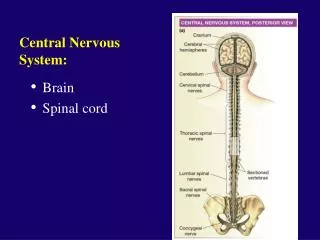
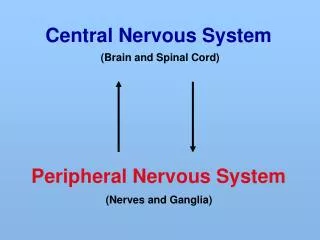
Surgical Terminology CNS lesions • BRAIN Intra-axial (Intra-parenchymal) Extra-axial (Extra-parenchymal) • SPINAL CORD Extradural Intradural Intramedullary Extramedullary
Diagnostic Methods • FNA • Touch imprints/ crush smears cytology • Stereotactic biopsy • Open surgery • Frozen section • Histopathology • CSF examination • CT Scan • MRI
MENINGITIS • Meningitis: an inflammatory process of leptomeninges and CSF in the subarachnoid space. • Meningoencephalitis: inflammation of brain parenchyma in addition to meninges. • Classification: • Acute pyogenic • Aseptic • Chronic
ACUTE PYOGENIC MENINGITIS CAUSATIVE ORGANISMS: Neonates:Escherichia coli, group B Streptococci, Hemophilus influenzae Young adults:Neisseria meningitis Elderly:Streptococcus pneumoniae, Listeria monocytogenes Clinical presentation: Systemic signs of infection, meningeal irritation, neurological impairment,, headache, photophobia, irritability, clouded consciousness, neck stiffness. Spinal tap: Cloudy or purulent CSF, increased pressure, neutrophil count raised to 90,000/mm3, raised protein levels, markedly decreased glucose levels. Smear may show bacteria on gram stain or culture
ACUTE PYOGENIC MENINGITIS Gross: Exudate over brain surface within the leptomeninges H.influenzae-exudate is basal; pneumococcal meningitis- exudate is over cerebral convexities near the sagittal sinus. Vessels engorged, pus tracts along blood vessels. Microscopy: neutrophils in subarachnoid space particularly around leptomeningeal blood vessels. Thrombosis of veins causes hemorrhagic infarction . Inflammatory infiltrate may track down through vessels to cause focal cerebritis Complications: Leptomaningeal fibrosis and hydrocephalus, chronic adhesive arachnoiditis
ACUTE ASEPTIC MENINGITIS Self limiting illness with no recognizable organism Etiology: Viral rarely bacterial. Viruses include enterovirus, echovirus, coxsackivirus, non paralytic polio virus. Spinal tap: lymphocytic pleocytosis, moderately elevated protein, normal sugar levels Microscopy: no pathology found except for occasional moderate brain swelling mild infiltration of leptomeninges with lymphocytes. DRUG INDUCED ASEPTIC MENINGITIS: NSAIDs and some antibiotic induced CHEMICAL MENINGITIS: subsequent to rupture of epidermoid cyst into subarachnoid space MENINGISM: postsurgical meningeal irritation dut to hemorrhages
CHRONIC MENINGITIS TUBERCULOSIS C/F: headache, malaise, confusion, vomiting Gross: gelatinous /fibrinous exudate in subarachnoid space, obliterating cisterns and encasing the cranial nerves. Discrete white granules over the leptomeninges. Microscopy: picture of diffuse meningoencephalitis , with lymphocytes , plasma cells, macrophages. Florid cases show granulomas, giant cells and caseation Obliterative end arteritis of subarachnoid vessels Dense fibrous adhesive arachnoiditis develops later. CSF: moderate pleocytosis, strikingly elevated protein levels, moderately raised or normal glucose. Tuberculoma: well circumscribed intraparenchymal mass measuring several cm, causing mass effect
Rickettsial Encephalitis Gross: swollen hyperemic brain, cloudiness of leptomeninges Microscopy: perivascular exudate mainly monocytes, typhus nodules– histiocytes, mononuclear cells In tertiary stage of syphilis-T.pallidum Meningovascular neurosyphilis Cerebral gumma General paresis of the insane Tabes dorsalis
FUNGAL INFECTIONS Cryotococcus neoformans : Most common CNS mycosis, seen in immuno suppressed. Microscopically: Ovoid spherical with mucicarmine capsule, replicates by budding from a narrow base.
MOLDS • Disseminated systemic mycosis: syndrome of multifocal stroke, occlusion, invasion, thrombosis of leptomeningeal and perforating cerebral vasculature. Infarcts colonized by fungi with limited inflammatory reaction or suppuration Morphology in tissue sections: • Solitary lesions: present as expanding intra cranial mass . Intact immune reseponse, • Abscess like or granulomatous lesion Aspergilus- stouter septate hyphae branch at frequent acute angles Mucoraceae –broad ribbon like nonseptate hyphae branch at right angles Rhinocerebral mucormycosis —associated with diabetic ketoacidosis, sepsis, uremia dehydration & other acidemic conditions, renal transplantation
DIMORPHIC FUNGI • Organisms: Blastomyces, Dermattidis, Histoplasma Capsulatum, Coccidiodes Immitis, Paracoccidiodes Braseliensis. • Chronic granulomatous meningitis with active systemic mycosis. Necrotizing granulomatous tissue replete with multinucleated giant cells. DERMATIACEOUS FUNGI • Organisms: pigmented hyphal yeast eg agents of madura foot and tinea capitis. • Cause neuroparenchymal lesions. CANDIDA INFECTIONS • Most common CNS mycosis in immunosuppressed patients • Small foci of suppuration scattered widely in the neuropil & occasional meningitis . Rarely granulomatous lesions/ micro abscess/ meningitis/ vasculitis occurs.
PARASITOSIS AMEBA Naegleria species-Necrotizing meningoencephalitis Acanthameba- Chronic granulomatous meningoencephalitis Cerebral Malaria Ring hemorrhages, Parasitized RBC’s Durck granulomas NEUROCYSTICERCOSIS Cysticercus cellulosae —larva of taenia solium Pathogenesis: Larvae encyst in brain skeletal muscle and ocular tissue. Host’s inflammatory response to larva’s death 18-months after primary infection. CT MRI: ring-enhancing cerebral cysts which resolves by antihelmintic treatment CSF or serological assays.
TOXOPLASMOSIS • Causative organism:Toxoplasma gondii - obligate intracellular protozoan • Predisposing conditions: most common space occupying lesion in AIDS , Bone marrow transplant recipients, Hodgkin disease • MRI CT:multifocal nodular lesion with ring-like peripheral enhancement edema and mass effect as solitary abscesses. • Serology: Serum antitoxoplasma IgG titer • Morphology: Abscesses consists of central mass of necrotic cellular debris surrounded by edema and inflammation, perivascular & intramural lymphoid infiltration , endothelial swelling, thrombosis, fibrinoid necrosis, toxoplasma seen in peripheral areas and rare in necrotic centre later fibrous obliteration of vessels . • Two protozoal forms: • Tachyzoite: injurious, faintly basophilic, 4-8um, crescentic shape.seen easily by toxoplasma specific antibodies • Bradyzoites: PAS positive, contained in membrane delimited true cysts, inert form in which parasite persists in chronically infected state.
Viral infections • Encephalitis-Perivascular and parenchymal mononuclear inflammatory infiltrate, microglial nodules, neuronophagia, viral inclusion bodies • Encephalomyelitis • Meningoencephalitis
HERPES SIMPLEX ENCEPHALITIS Clinical features: fever , lethargy, ataxia, seizures, altered consciousness CSF examination: pleocytosis, xanthochromia, assay for HSV specific antigens, PCR CT MRI: localized lesions in frontotemporal lobe. Morphology: Eosinophilic intranuclear inclusion bodies in neurons and glia Late stage: 2nd week, lymphocytes plasma cells colonize the meninges, microglial nodules of mono nuclear cells around affected neurons, Hemorrhage , thrombosis & fibrinoid necrosis may be seen. Later foamy macrophages clear the debris with formation of cavitated gliotic remnants. Electron microscopy: HSV particle in nucleus Immunohistochemical analysis: commercially available antibodies to HSV.
SUBACUTE SCLEROSING PANENCEPHALITIS • Cause: Persistent nonproductive infection of CNS by an altered measles virus • Clinical features :cognitive decline, spasticity , seizures. Occurring months or years after acute measles infection • Morphology: Wide spread gliosis degeneration . • Viral inclusions within nuclei of oligodendrocytes & neurons and neurofibrillary tangles. • E/M: nucleocapsids , characteristic of measles virus. • Immuno: virus antigen positive
PROGRESSIVE MULTIFOCAL LEUKOENCEPHALOPATHY • Organism: JC polyoma virus. • Pathogenesis: No clinical disease with primary infection. PML results from reactivation of virus as a result of defective cell mediated immunity. eg in AIDS, chronic lympho- proliferative or myeloproliferative illness • Site: mainly cerebral hemispheres white matter cerebellar and bulbar localization less common and spinal cord is spared • Morphology: Virus mainly infects oligodendrocytes, resulting in progressive demyelination of neurons , mostly in subcortical location. Lipid laden macrophages & reduced number of axons in the centre .At periphery greatly enlarged oligodendrocytes with basophilic ground glass amphophilic nuclei • Immunohistochemistry: viral antigens in the oligodendrocytes • Clinical features: motor deficits , cognitive decline, visual loss. • CT MRI: scattered foci of white matter hypodensity unassociated with mass effect or contrast enhancement. • CSF exam: detection of JC-virus DNA by PCR.
large "ballooned" oligodendrocytes infected with JC virus with enlarged dark pink "ground glass" nuclei containing viral antigen
HUMAN IMMUNODEFICIENCY VIRUS • VACUOLAR MYELOPATHY: 20%-30% of patient • Subacute combined degeneration with normal vit B 12 levels. • AIDS-ASSOCIATED MYOPATHY : inflammatory myopathy • Subacute onset of proximal weakness, pain, raised CK levels • Morphology: Muscle fiber necrosis& phagocytosis, interstitial infiltration with HIV-positive macrophages, • Acute toxic reversible myopathy with ragged red fibers and myoglobulinuria in patients with AZT treatment.
CYTOMEGALOVIRUS • Occurs in fetuses & immunosuppresed individuals. • In utero infection: periventricular necrosis, severe brain destruction , followed by microcephaly and periventricular calcification • Immunosuppressed patients: subacute encephalitis with tropism for paraventricular subependymal regions • Results in severe necrotizing ventriculoencephlitis & choroid plexitis • Prominent cytomegalic cells with intranuclear and intracytoplasmic inclusions
POLIOMYELITIS • Causative organism: Picorna group of enteroviruses. secondarily invades CNS • Clinical features; meningeal irritation, flaccid paralysis, muscle wasting and hyporeflexia • CSF exam: aseptic meningitis • Morphology: Mononuclear cell perivascular cuffs and neuronophagia of anterior horn motor neurons , cavitation and gliosis.
RABIES • Clinical features: incubation period depends on distance b/w wound and the brain. • Malaise , headache, fever, local parasthesias around the wound,. Later there is severe CNS excitability, convulsions, contracture of pharyngeal muscles, hydrophobia , foaming of mouth, meningismus. • later flaccid paralysis, stupor, comma, death from respiratory failure. • Morphology: Intense edema vascular congestion, widespread neuronal degeneration , inflammatory reaction most sever in Rhombencephalon • Negri bodies—cytoplasmic round to oval, eosinophilic inclusions, in pyramidal neurons of Hippocampus and Purkinje cells of cerebellum
TRANSMISSIBLE SPONGIOFORM ENCEPHALOPATHIES • Includes CJD, grstmann-Straussler-Scheinker syndrome, fatal familial insomnia, kuru in humans, mink transmissible encephalopathy, • All associated with abnormal forms of transmissible and infectious proteins—prion protein PrP • Genetics: gene PRNP for PrPsc on chromosome 20 , has high degree of conservancy among species • Pathogenesis: conformational change in PrPsc αhelix containing isoform to β-pleated sheet isoform PrPres –leads to resistance to proteases • PrPsc accumulates in neural tissue • Clinical features: dementia, • Western blotting of tissue extracts used for diagnostic detection of PrPsc
TRANSMISSIBLE SPONGIOFORM ENCEPHALOPATHIES • Microscopy: multi focal spongiform transformation of cerebral cortex along with deep nuclei • Formation of empty vacuoles in the neuropil or perikaryon. • Neuronal loss, reactive gliosis, cystic spaces in advanced cases. • No inflammatory infiltrate is present • Electron microscopy :vacuoles are intracytoplasmic and membrane bound in neuronal processes • Kuru plaques extra cellular congo red and PAS + deposits composed of aggregated abnormal protein • Immunohistochemistry: demonstration of protein K resistance PrPsc in tissue
Acute disseminated encephalomyelitis • ADEM monophasic demyelinating disease • Cause: viral infection or viral immunization • Clinical features: diffuse headaches, lethargy, coma, • Morphology: Milder disease, gray discoloration of white matter around vessels. • Myelin loss with preservation of axons and lipid laden macrophages Acute necrotizing hemorrhagic encephalomyelitis • Effects young adults & children after an episode of upper respiratory infection • Morphology: Perivenular distribution of demyelination and widespread dissemination. • Destruction of small blood vessels, disseminated necrosis, acute hemorrhage, fibrin deposition, abundant neutrophils and lymphocytes.
BRAIN ABSCESS • Predisposing conditions: Pyogenic extraneural infections, anatomic anomalies, penetrating cranial trauma, neurosurgery • 20% without any predisposing history. • LOCAL EXTENSION: • Retrograde thrombophlebitic carriage from infections of Paranasal sinuses, middle ear, mastoid through emissray veins • Organisms: streptococcus intermedius group, aerobic gram negative bacilli- proteus, escherichia coli, klebsiella , enterobacter haemophilius species. • Odontogenic abscesses • Organisms:fusobacterium, bacteroides, streptococcus species. • Facial scalp infections • Organisms: streptococci, actinomyces
BRAIN ABSCESS • HEMATOGENOUS SEEDING: • multiple abscesses, commonly lying in the territories of middle cerebral arteries, germinating at gray white matter junction, and also cerebellum, basal ganglia, thalami, brain stem. • Origin: thorax—lung abscess, bronchiectasis Bacterial endocarditis, empyema, osteomyelitis, deep pelvic infections. • Other causes: cyanotic congenital heart diseases, polycythemia, hereditary hemorrhagic telangiectasia, iatrogenic causes like surgery, esophageal instrumentation • DIRECT INOCULATION: • by penetrating trauma or neurosurgery - least frequent, • Organisms:S. Aureus, Streptococus, Enterrobaceter, Closteridum species, Salmonella
BRAIN ABSCESS • Clinical features: headache, altered mental status, focal sensorimotor deficits, seizure, nausea, vomiting. • CSF tap: increased pressure, raised WBC count & proteins, normal sugar levels. • CT MRI shows central hypodensity, ring enhancement and characteristic surrounding edema. • Microscopy:ill defined zones of bacterial multiplication, and cerebritis, commonly situated in gray white junction or in white matter subjacent to cortical ribbon. • Later fibroblasts proliferate, form a collagenous capsule surrounding a mass of fibinopurulent debris.Edematous inflamed gliotic brain tissue surrounds the capsule • In hematogenous seeding capsules are less well developed and have greater tendency for daughter abscesses, which rupture into ventricular system
WHO CLASSIFICATION OF CNS TUMORS (Modified) ASTROCYTIC TUMORS:( Gliomas) • Fibrillary (diffuse) astrocytoma - Grade II • Anaplastic astrocytoma – Grade III • Glioblastoma (G.Multiforme) – Grade IV • Pilocytic astrocytoma – Grade I • Pleomorphic xanthoastrocytoma - Grade II OLIGODENDROGLIAL TUMORS: • Oligodendroglioma • Anaplastic oligodendroglioma
WHO CLASSIFICATION OF CNS TUMORS EPENDYMAL TUMORS: • Ependymoma • Anaplastic ependymoma • Myxopapillary ependymoma CHOROID TUMORS: • Choroid plexus papilloma • Choroid plexus Carcinoma GLIAL TUMORS of UNCERTAIN ORIGIN: • Astroblastoma
WHO CLASSIFICATION OF CNS TUMORS NEURONAL & MIXED NEURONAL-GLIAL TUMORS: • Gangliocytoma • Ganglioglioma NEUROBLASTIC TUMORS: • Olfactory neuroblastoma PINEAL TUMORS: • Pineocytoma • Pineoblastoma EMBRYONAL TUMORS: • Medulloblastoma • PNET • Neuroblastoma
WHO CLASSIFICATION OF CNS TUMORS TUMORS OF MENINGOTHELIAL CELLS: • Meningioma • Anaplastic Meningioma TUMORS OF UNCERTAIN HISTOGENESIS: • Hemangioblastoma LYMPHOMAS HEMATOPOIETIC NEOPLASM: • Lymphoma • Plasmacytoma MESENCHYMAL TUMORS e.g, Lipoma, Liposarcoma, Leiomyoma, Leiomyosarcoma,Ostesarcoma
WHO CLASSIFICATION OF CNS TUMORS GERM CELL TUMORS: • Germinoma • Embryonal carcinoma • Yolk sac tumor • Choriocarcinoma • Teratoma TUMORS OF SELLAR REGION: • Craniopharyngioma TUMORS OF PERIPHERAL NERVES: • Schwannoma • Neurofibroma • MPNST METASTATIC TUMORS: e.g Ca lung, breast, prostate, melanoma, lymphoma, leukemia
ASTROCYTOMA • Infiltrating neoplasm composed of fibrillary or fibrous astrocytes • Constitute the most common primary CNS tumor • Extend over a continuous, morphologic spectrum of differentiation and grade • Associated with radiation, type1 neurofibromatosis, Li-Fraumeni syndrome, Turcot syndrome, Ollier or Maffucci disease Age and site: Any age, in adults more in cerebral hemispheres • Pediatric population in brain stem • Less common in spinal cord S/S: headache, seizures, focal sensorimotor deficit , Progressive cranial nerve and long tract dysfunction in brain stem lesions
PROGNOSIS • Depends on age, functional status on presentation, tumor location and histology • Good prognosis-young, cerebral hemispheres lesions, no focal neurological deficit and low grade tumors • Bad prognosis-anaplastic astrocytoma, GBM, diffusely infiltrative astrocytoma of brainstem • Survival for grade II- 5 yrs • Survival for grade III- 2-5 yrs • Survival for grade IV- <1 yr • Proliferative potential of tumor is determined by MIB 1 labelling index