
HEMOGLOBIN
E N D
Presentation Transcript
Hemoglobin M.Prasad Naidu MSc Medical Biochemistry, Ph.D.Research Scholar
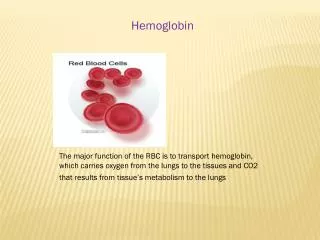
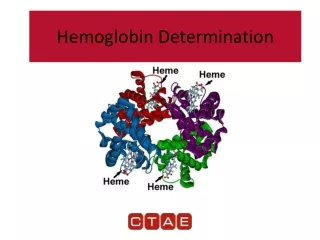
Hemoglobin (Hb) Hemoglobin is the red blood pigment exclusively found in erythrocytes. Normal range: Concentration of Hb in blood in Males is 14 – 16 g/dl Females is 13 – 15 g/dl
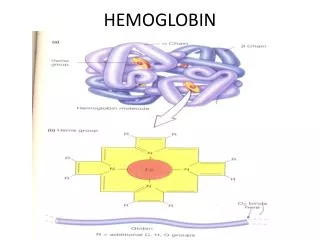
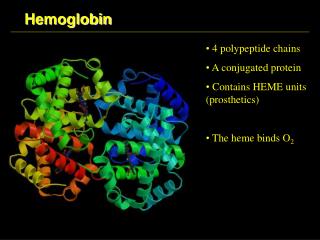
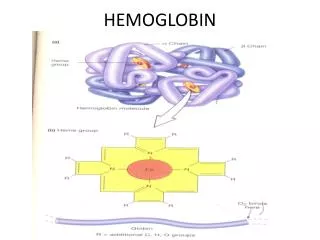
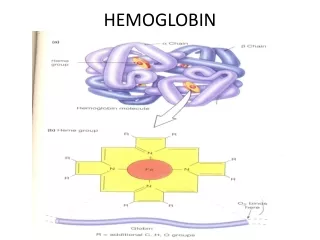
Structure: Tetrameric allosteric protein • Mol wt 64,450 • Conjugated protein globin +heme • Globin is the apoprotein part • Heme is the non-protein part (Prosthetic part) • Chromo protein • Example of quaternary structure of protein • Globular protein • Consist of 4 poly peptide chain 2 of one type and 2 of another type ( α2 and β2) held together by noncovalent bonds.
αhelical conformation constitutes 75% globin molecules. • 4 of helices are terminated by proline residues. • Each polypeptide chain contains heme group and oxygen binding cite. • Heme consist of protoporphyrin ring and Fe atom • Fe atom in heme can forms 6 bonds. • 4with N of protoporphyrin • 5th one imidazole N of proximal histidine. • In OxyHb , 6th binds to O2
Function: 1.Delivery of O2 from the lungs to the tissues 2. Transport of CO2 and protons (H+) from tissue to lungs for expiration.
Effect of 2,3,BPG on O2affinity of Hb levels are higher in younger children compared to elders. 2,3 BPG is produced in the erythrocytes from an intermediate (1,3 Bisphosphoglycerate) of glycolysis. This short pathway is refered as Rapaport Leubering cycle.
Significance of Rapaport leubering cycle It prevents accumulation of ATP not needed by the erythrocyte It supplies 2,3 BPG in oxygen transport which is required for the Hb function. 2,3 BPG regulates the binding and release of Oxygen from hemoglobin. 2,3 BPG accounts for about 16% of the non carbonate buffer value of erythrocyte fluid.
HEME Iron containing compound belonging to the class of protoporphyrin compounds Protoporphyrin is composed of 4 pyrrole rings which are linked by methene (=CH) bridges to from tetrapyrrole (porphyrin) 4 methyl , two vinyl and two propionate side chain gps are attached to the porphyrin rings.
These can be arranged in 15 different ways One of these isomers called protoporphyrin IX is biologically active. Iron (Fe2+) held in the center of the protoporphyrin molecule by co-ordination bonds with the four nitrogen of the protoporphyrin ring.
Iron has 6 valency • 4 bonds are formed b/n iron and nitrogen atoms of the porphyrin ring system • 5th bond is formed between nitrogen atom of histidine residue of the globin polypeptide chain, known as proximal histidine. • 6th bond is formed with oxygen
Heme Synthesis Takes place in all cells (occurs to the greatest extent in the bone marrow and liver) Occurs both in mitochondria and cytosol.
Stages of Heme Synthesis 1.Biosynthesis of - aminolevulinic acid (ALA) from the precursor glycine and succinyl CoA 2.Formation of porphobilinogen (PBG) from δ amino levulinic and 3. conversion of the porphobilinogen to the cyclic tetrapyrrol porphyrin ring and heme.
Biosynthesis of δ ALA • 1st step is biosynthesis of Heme • Condensation step (succinyl CoA + glycine) • Rate controlling step in heme synthesis • Occurs in mitochondria
Formation of PBG Occurs in cytosol 2 mol of δ ALA condense to form one mol of porphobilinogen ad 2H2O. Enzyme is ALA dehydratase , Zn containing enzyme. Enzyme is inhibited by lead and ALA is excreted in urine (lead poisoning).
Conversion of porphobilirogen to porphyrins and heme 4 BPG condense head to tail to form a linear tetrapyrrole. Enzyme is PBG deaminase. PBG cylized spontaneouusly to form UPGI and UPG III , Enzyme is UPG III cosynthase UPG III is converted to CPG III by decarboxylation of all acetate(A) side chain to methyl (M), enzyme is UPG decarboxylase. CPG III enter mitochondria , it is converted to PPG III by CPG oxidase enzyme.
This enzyme catalyzed the conversion of two of the proprionate side chains into vinyl groups by oxidative decarboxylation. This enzyme act only on type III coproporphyrinogen Oxidation of protoporphyrinogen III to protoporphyrin is catalyzed by another mitochondrial enzyme, protoporphyrinogen oxidase.
Final step involves the incoporation ferrous iron into protoporphyrin in a reaction catalyzed by mitochondrial heme synthase or ferrochelatase
Regulations of Heme Synthesis 1.ALA synthase allosteric enzyme that catalyzed controlling step, feed back inhibition by Heme. 2.Iron atom itself may be the active regulatory species 3.Several substances like steroid hormone metabolites ethanol, Barbiturate etc induce the synthesis of hepatic ALA
Disorders of Heme biosynthesis Porphyrias
Breakdown of Hemoglobin RBC life span is 120 days , after this they are degraded by RE system
Fate of Bilirlubin Metabolism & excretion of bilirubin occurs in liver & intestine • Uptake by liver parenchymal cells • Conjugation in smooth endoplasmic reticulum in liver • Secretion of conjugated bilirubin • Excretion of bilirubin in the form of stercobilin and urobilinogen through feces and urine respectively
Disorders of Hemoglobin Catabolism Normal concentration of serum bilirubin • Total bilirubin 0.1 - 1.0 mg/dl • Conjugated (direct) bilirubin 0.1 – 0.4 mg/dl • Unconjugated (indirect)bilirubin 0.2 – 0.8 mg/dl • Bilirubin in blood morethan 1mg/dl is called clinical hyperbilirubinemia.
Hyper bilirubinemia : • Increased bilirubin production • Decreased hepatic uptake • Decreased hepatic conjugation • Decreased excreation of bilirubin into bile • Bilirubin accumulates in allthese conditions approximately 2.2 - 5 mg/dl. • The skin and sclere appears yellowish due to deposition of bilirubin in the tissue. • The condition is called jaundice or Icterus.
Jaundice: (Hyperbilirubimia) acquired or inherited Conjugated or Unconjugated 4 types • Hemolytic or prehepatic • Hepato cellular / Hepatic / intrahepatic • Obstructive / Post hepatic • Neonatal / Physiological jaundice
Acquired hyperbilirubimia • Prehepatic or Hemolytic eg: - sickle haemoglobin (sickle cell anemia) - deficiency of enzyme glucose 6-phosphate dehydrogenase. - Incompatible blood transfusion Biochemical features • Increased plasma unconjugated bilirubin • Increased amount of urobilinogen in urine and Feces. • Absence of bilirubin in urine.
Intrahepatic / Hepatic / Hepatocellular Jaundice Infection (viral hepatitis) Toxic chemicals (alcohol) Drugs cirrhosis • Uncojugated hyperbilirubinemia and presence of some conjugated hyperbilirubinemia Biochemical Features • Increased plasma concentrtaion of conjugated and unconjugated bilirubin. • Decreaed amount of urobilinogen in urine and faeces • Presence of bilirubin in the urine • Raise level of alanine transaminase enzyme
Posthepatic or Obstructive Jaundice occurs due to obstruction in the passage of conjugated bilirubin from the liver cells to the intestine this condition is also called as cholestasis. Causes • Blockage of common bile duct by gallstones • Carcinoma of the head of the pancreas • carinoma of the duct
Biochemical Features: Increased conjugated bilirubin in plasma Absence of urobilinogen in faeces and urine Presence of bilirubin and bile salts in urine Raised ALP in plasma
Neonatal of physiologic jaundice • Mild jaundice in the first few days after birth • Results from an accelerated haemolysis and immature liver enzyme system for conjugation • Liver is deficient in enzyme UDP-glucuronyl transferase. • Increased unconjugated bilirubin is seen • If it exceeds 20 – 25 mg/dl it penetrates the BBB • This results in hyperbilirubinaemic toxic encephalopathy or kernicterus
Inherited hyperbilirubinaemia • Gilbert’s syndrome • Crigler Najjar syndrome • Dubin Johnson syndrome • Rotor syndrome