Download
1 / 59
620 likes | 1.05k Vues
Nursing Care of Individual with Genitourinary Disorders: Renal Trauma Renal Vascular Problems Acute Renal Failure. a. Fibrous capsule b. Renal cortex c. Renal medulla d. Pyramids e. Papillae f. Minor calyx g. Major calyx h. Renal pelvis i. Ureter. I. A&P of the Kidney.

E N D
Nursing Care of Individual with Genitourinary Disorders:Renal TraumaRenal Vascular ProblemsAcute Renal Failure
a. Fibrous capsule b. Renal cortex c. Renal medulla d. Pyramids e. Papillae f. Minor calyx g. Major calyx h. Renal pelvis i. Ureter I. A&P of the Kidney
Renal A & P Review:
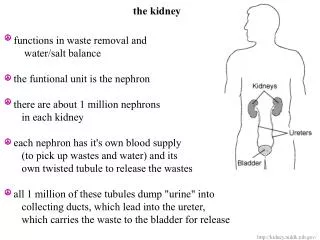
Elimination of _______ & _________ • Can you name some of these substances? __________________________ • Regulates fluid & electrolyte balance thru processes of: __________, _________, and _____________. II. Functions of the Kidneys
Name a few of these Fluid and Electrolyes regulated by kidneys __________________ __________________ __________________ Functions of the Kidneys (continued)
Regulates acid-base balance • HCO3 and H+ • Hormonal (endocrine) functions: • Renin Release Functions of the Kidneys (cont)
Erythropoietin Release • If a patient has chronic kidney disease or chronic renal failure, what condition will occur and WHY??? Functions of the Kidneys (cont)
Activated Vitamin D • Necessary to absorb Calcium in the GI tract. There is decrease in synthesis of D3, the active metabolite of Vitamin D If a patient has renal failure, what will happen to the patient’s serum calcium level? __________________ Functions of the Kidneys (cont)
Why is it called the functional unit of the Kidney??? III. The Nephron
a. Glomerulus • b. Bowman’s capsule • c. Proximal tubule • d. Loop of Henle • e. Distal tubule • f. Collecting duct Label the Nephron’s Parts
Etiology: • Blunt force from falls, MVA, sports injuries, knife/gunshot wounds, impalement injury, rib fractures Renal Trauma
Common Manifestations: • Microscopic to gross hematuria • Flank or abdominal pain • Oliguria or anuria • Localized swelling, tenderness, ecchymosis flank area • Turner’s sign=bluish discoloration flank area due to retroperitoneal bleeding Renal Trauma
What are some diagnostic tests used in renal trauma? • IVP, renal ultrasound, CT scan, renal arteriogram • What serum levels can be useful? • _________________________ Renal Trauma
You are a student nurse on day shift and you hear in report that your patient is scheduled to have an IVP this am…. What do you know about an IVP? What do you teach the patient about preparing for this procedure? What nursing interventions or orders should you anticipate? Clinical scenario
Bedrest and close observation. • Monitor for S & S of what??? ____________________ • Embolization or open surgery to stop bleeding or repair • Partial or total Nephrectomy Renal Trauma-Interventions
Indications for Nephrectomy: • Renal tumor • Massive Trauma • Polycystic Kidney Disease • Donating a Healthy kidney Renal Surgery-Nephrectomy
Post Op Nursing Management • Strict I & O • Urine output should be at least _____. • What should u.o. be if patient had bilateral nephrectomy? ______. • Observe ACC of urine. • TCDB & incentive spirometry • Incision in flank area, 12th rib removed • Medicate for pain as ordered Renal Surgery-Nephrectomy
I. Hypertension & Nephrosclerosis • Sustained elevation of the systemic blood pressure can result from or cause kidney disease---How? Renal Vascular Problems
Development of arterio sclerotic lesions in the arterioles and glomerular capillaries ↓ Decreased blood flow which leads to ischemia and patchy necrosis ↓ Destruction of glomeruli ↓ Decrease in GFR Patho of HTN-Nephrosclerosis
Definition: Narrowing of one or both renal arteries due to atherosclerosis or structural abnormalities. • Common Manifestations: • Uncontrollable HTN Renal Vascular Problems II. Renal Artery Stenosis
How could a renal artery stenosis result in HTN? Critical thinking question…
Treatment/Collaborative Care • Anti-hypertensive Medications • Dilation of renal artery by Percutaneous Transluminal Angioplasy • Bypass Graft of Renal Artery • Stent placement Renal Artery Stenosis
Treatment/Collaborative Care Renal Artery Stenosis
Definition: rapid decline in renal function that leads to accumulation of nitrogenous wastes (azotemia) • Etiology of ARF: • Pre-renal • Intra-renal • Post renal Acute Renal Failure
What is missing from the ARF definition? What is the difference between uremia and azotemia??? ____________________________ Compare & Contrast…
Etiology of Acute Renal FailurePre-renal • List causes of “pre-renal” ARF failure-all related to decreased blood flow to the kidneys • Hypovolemia: dehydration, shock, burns • Decreased cardiac output: CHF, MI, arrythmias • Renal vascular obstruction: renal artery stenosis, or renal artery blockage.
Etiology of Acute Renal FailureIntra-renal • Direct injury to the kidneys • Conditions causing direct insult to renal tissue causing damage to nephrons • List causes of “intra renal” ARF failure:
Causes of Intrarenal Failure • Primary renal disease: acute glomeulonephritis and acute pyelonephritis • ATN (Acute tubular necrosis) most common causes • Result from ischemia, nephrotoxins, (such as antibiotics), hemoglobin released from hemolyzed red blood cells, or myoglobin released from necrotic muscle cells
Frequent causes of “intra-renal” failure • ATN: acute tubular necrosis of tubular cells which slough and plug tubules (nephrotoxicity, ischemia); potentially reversible • Hemolytic blood transfusion (ATN) • Trauma (crushing injuries which release myoglobin; damaged muscle tissue and blocks tubules (rhabdomylosis)(ATN) • What is Rhabdomylosis?
Nephrotoxic drugs/chemicals (ATN) • Aminoglycosides* • Radiographic contrast agents • Arsenic, lead, carbon tetachloride • Acute glomerulonephritis/pyelonephritis • Systemic lupus
Causes of Acute Renal Failure (ATN) • Renal ischemia • Disruption basement membrane;destruction tubular epithelium • Nephrotoxic agents • Necrosis tubular epithelium… plug tubules; basement membrane intact. • Potentially reversible IF • Basement not destroyed and tubular epithelium regenerates Renal ischemia Nephrotoxic agents
Identify three causes of “post-renal failure” (mechanical obstruction of urinary outflow; urine backs up into renal pelvis) • BPH (Benign Prostatic Hypertrophy) • Calculi • Trauma • Prostate cancer Etiology of Acute Renal Failure Post-renal
Diagnostic Tests in Acute Renal Failure: • BUN (blood urea nitrogen) • Normal = please change to 6-20 mg/dl; measurement of amount of urea in blood • What is urea?_____ • BUN fluctuates • BUN elevated in______; decreased in_________.
Which of the following urinary symptoms is the most common initial manifestations of ARF? a-dysuria b-anuria c-hematuria d-oliguria Question…
The client’s BUN is elevated in ARF. What is the likely cause of this finding? • a-fluid retention • b-hemolysis of red blood cells • c-below normal protein intake • d-reduced renal blood flow Question…
Another client is scheduled to get a CT with contrast of their abdomen and is at risk for ARF. The physician has prescribed acetylcysteine (Mucomyst) 5% 20ml po prior to CT scan. The nurse proceeds to look up the medication and sees that the drug is a mucolytic. The patient has no history of respiratory disease. Why is this patient receiving this medication? CLINICAL SCENARIO
You are the Level 4 nursing student assigned to a group of patients. One of the patients is taking glucophage 500mg orally every morning. What does the RN need to know prior to administration of this medication? Another client is scheduled to get a CT with contrast of their abdomen and is at risk for ARF, what does the RN need to know? Clinical scenario
The RN is taking care of a group of patients. One of the patients is taking glucophage 500mg orally every morning. What does the RN need to know prior to administration of this medication? Another client is scheduled to get a CT with contrast of their abdomen and is at risk for ARF, what does the RN need to know? Activity
Diagnostic Tests in Acute Renal Failure: • Serum Creatinine: end product of muscle and protein metabolism; excreted by the kidneys at a constant rate • Normal = 0.6-1.3 mg/dl please change this value on your ppt • Directly related to GFR • 2 X normal (2.6) = 50% nephron fx loss • 10 X normal (13) = 90% nephron fx loss • MORE ACCURATE INDICATOR of RENAL FUNCTION THAN BUN • BUN; Creatinine ratio Normal= 10:1 BUN Creatinine 16 1.6 12 1.2
Diagnostic Tests in Acute Renal Failure: • Creatinine clearance • Most accurate indicator of Renal Function • Reflects GFR • Involves a 24 hr urine/serum creatinine • Formula: Amount of urine creatinine X urine V serum creatinine • Normal= 100-135ml/minute
A 24 hours urine for creatinine clearance is ordered for Ms. J. Which task is appropriate to delegate to the the clinical assistant? a) instruct Ms. J to collect all urine with each voiding b) explain the purpose of collecting a 24 hour urine c) ensure that the 24 hour urine collection is kept on ice d) assess Ms. J’s urine for color, odor, sediment Question…..
Diagnostic Tests in Acute Renal Failure: • Urine Specific Gravity • Normal= 1.003-1.030 • Will be fixed a 1.010 usually in ARF due to kidneys losing ability to concentrate urine • Serum Electrolytes 1- Serum Sodium Normal= 135-145 • May be high, low, or normal • High in Volume deficit (dehydration) • Low due to damaged tubules not conserving sodium
Diagnostic Tests in Acute Renal Failure: • Serum Electrolytes 2- ↑ Serum K+ Normal= 3.5-5.0 meq/l • Almost always increased • WHY? • Kidneys excrete 80-90% of our K+ • If K+> 6.0; treatment initiated to prevent ______________________
Diagnostic Tests in Acute Renal Failure: • Serum Electrolytes 3- ↑ Serum Phosphorus Normal= 2.8-4.5mg/dl Phosphorus is a product of protein breakdown excreted by the kidneys What other process is occurring to increase serum phosphorus??? __________________
Diagnostic Tests in Acute Renal Failure: • Serum Electrolytes 4 - ↓ Serum Calcium Normal= 9.0-11.0 mg/dl due to ↓ production of activated Vitamin D; Vitamin D needed to absorb calcium from GI tract What other process is occurring to decrease serum calcium??? __________________
Diagnostic Tests in Acute Renal Failure: • ABGs • pH • Metabolic acidosis due to ability of kidneys to excrete acid metabolites (uric acid) so the pH will be __________. • Also, bicarb levels due to bicarb being used up to buffer excess H+ ions.
Treatment During: Oliguric/Non-Oliguric Phase • Fluid Challenge/Diuretics • Done to r/o dehydration as cause of ARF and to blast out tubules if ATN. • 250-500cc NS given I.V. over 15 minutes • Mannitol (osmotic diuretic) 25gm I.V. given • Lasix 80mg I.V. given • Should see what within 1-2 hours????
Treatment During: Oliguric/Non-Oliguric Phase • If fluid challenge fails, fluid intake is usually limited and client is placed on fluid restriction • Restriction is limited to 600ml + u.o. past 24 hours • Physician will specify in the orders how much. Question: Patient’s u.o. on Tuesday=300ml, what will be his fluid intake allowed on Wednesday? ________